Nishani Jayasooriya, Sonia Saxena, Jonathan Blackwell, Alex Bottle, Hanna Creese, Irene Petersen, Richard C G Pollok
{"title":"炎症性肠病患者之前使用医疗服务、确诊时间与临床结果之间的关系:一项具有全国代表性的人群队列研究。","authors":"Nishani Jayasooriya, Sonia Saxena, Jonathan Blackwell, Alex Bottle, Hanna Creese, Irene Petersen, Richard C G Pollok","doi":"10.1136/bmjgast-2024-001371","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Timely diagnosis and treatment of inflammatory bowel disease (IBD) may improve clinical outcomes.</p><p><strong>Objective: </strong>Examine associations between time to diagnosis, patterns of prior healthcare use, and clinical outcomes in IBD.</p><p><strong>Design: </strong>Using the Clinical Practice Research Datalink we identified incident cases of Crohn's disease (CD) and ulcerative colitis (UC), diagnosed between January 2003 and May 2016, with a first primary care gastrointestinal consultation during the 3-year period prior to IBD diagnosis. We used multivariable Cox regression to examine the association of primary care consultation frequency (n=1, 2, >2), annual consultation intensity, hospitalisations for gastrointestinal symptoms, and time to diagnosis with a range of key clinical outcomes following diagnosis.</p><p><strong>Results: </strong>We identified 2645 incident IBD cases (CD: 782; UC: 1863). For CD, >2 consultations were associated with intestinal surgery (adjusted HR (aHR)=2.22, 95% CI 1.45 to 3.39) and subsequent CD-related hospitalisation (aHR=1.80, 95% CI 1.29 to 2.50). For UC, >2 consultations were associated with corticosteroid dependency (aHR=1.76, 95% CI 1.28 to 2.41), immunomodulator use (aHR=1.68, 95% CI 1.24 to 2.26), UC-related hospitalisation (aHR=1.43, 95% CI 1.05 to 1.95) and colectomy (aHR=2.01, 95% CI 1.22 to 3.27). For CD, hospitalisation prior to diagnosis was associated with CD-related hospitalisation (aHR=1.30, 95% CI 1.01 to 1.68) and intestinal surgery (aHR=1.71, 95% CI 1.13 to 2.58); for UC, it was associated with immunomodulator use (aHR=1.42, 95% CI 1.11 to 1.81), UC-related hospitalisation (aHR=1.36, 95% CI 1.06 to 1.95) and colectomy (aHR=1.54, 95% CI 1.01 to 2.34). For CD, consultation intensity in the year before diagnosis was associated with CD-related hospitalisation (aHR=1.19, 95% CI 1.12 to 1.28) and intestinal surgery (aHR=1.13, 95% CI 1.03 to 1.23); for UC, it was associated with corticosteroid use (aHR=1.08, 95% CI 1.04 to 1.13), corticosteroid dependency (aHR=1.05, 95% CI 1.00 to 1.11), and UC-related hospitalisation (aHR=1.12, 95% CI 1.03 to 1.21). For CD, time to diagnosis was associated with risk of CD-related hospitalisation (aHR=1.03, 95% CI 1.01 to 1.68); for UC, it was associated with reduced risk of UC-related hospitalisation (aHR=0.83, 95% CI 0.70 to 0.98) and colectomy (aHR=0.59, 95% CI 0.43 to 0.80).</p><p><strong>Conclusion: </strong>Electronic records contain valuable information about patterns of healthcare use that can be used to expedite timely diagnosis and identify aggressive forms of IBD.</p>","PeriodicalId":9235,"journal":{"name":"BMJ Open Gastroenterology","volume":"11 1","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11131120/pdf/","citationCount":"0","resultStr":"{\"title\":\"Associations between prior healthcare use, time to diagnosis, and clinical outcomes in inflammatory bowel disease: a nationally representative population-based cohort study.\",\"authors\":\"Nishani Jayasooriya, Sonia Saxena, Jonathan Blackwell, Alex Bottle, Hanna Creese, Irene Petersen, Richard C G Pollok\",\"doi\":\"10.1136/bmjgast-2024-001371\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Timely diagnosis and treatment of inflammatory bowel disease (IBD) may improve clinical outcomes.</p><p><strong>Objective: </strong>Examine associations between time to diagnosis, patterns of prior healthcare use, and clinical outcomes in IBD.</p><p><strong>Design: </strong>Using the Clinical Practice Research Datalink we identified incident cases of Crohn's disease (CD) and ulcerative colitis (UC), diagnosed between January 2003 and May 2016, with a first primary care gastrointestinal consultation during the 3-year period prior to IBD diagnosis. We used multivariable Cox regression to examine the association of primary care consultation frequency (n=1, 2, >2), annual consultation intensity, hospitalisations for gastrointestinal symptoms, and time to diagnosis with a range of key clinical outcomes following diagnosis.</p><p><strong>Results: </strong>We identified 2645 incident IBD cases (CD: 782; UC: 1863). For CD, >2 consultations were associated with intestinal surgery (adjusted HR (aHR)=2.22, 95% CI 1.45 to 3.39) and subsequent CD-related hospitalisation (aHR=1.80, 95% CI 1.29 to 2.50). For UC, >2 consultations were associated with corticosteroid dependency (aHR=1.76, 95% CI 1.28 to 2.41), immunomodulator use (aHR=1.68, 95% CI 1.24 to 2.26), UC-related hospitalisation (aHR=1.43, 95% CI 1.05 to 1.95) and colectomy (aHR=2.01, 95% CI 1.22 to 3.27). For CD, hospitalisation prior to diagnosis was associated with CD-related hospitalisation (aHR=1.30, 95% CI 1.01 to 1.68) and intestinal surgery (aHR=1.71, 95% CI 1.13 to 2.58); for UC, it was associated with immunomodulator use (aHR=1.42, 95% CI 1.11 to 1.81), UC-related hospitalisation (aHR=1.36, 95% CI 1.06 to 1.95) and colectomy (aHR=1.54, 95% CI 1.01 to 2.34). For CD, consultation intensity in the year before diagnosis was associated with CD-related hospitalisation (aHR=1.19, 95% CI 1.12 to 1.28) and intestinal surgery (aHR=1.13, 95% CI 1.03 to 1.23); for UC, it was associated with corticosteroid use (aHR=1.08, 95% CI 1.04 to 1.13), corticosteroid dependency (aHR=1.05, 95% CI 1.00 to 1.11), and UC-related hospitalisation (aHR=1.12, 95% CI 1.03 to 1.21). For CD, time to diagnosis was associated with risk of CD-related hospitalisation (aHR=1.03, 95% CI 1.01 to 1.68); for UC, it was associated with reduced risk of UC-related hospitalisation (aHR=0.83, 95% CI 0.70 to 0.98) and colectomy (aHR=0.59, 95% CI 0.43 to 0.80).</p><p><strong>Conclusion: </strong>Electronic records contain valuable information about patterns of healthcare use that can be used to expedite timely diagnosis and identify aggressive forms of IBD.</p>\",\"PeriodicalId\":9235,\"journal\":{\"name\":\"BMJ Open Gastroenterology\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11131120/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjgast-2024-001371\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjgast-2024-001371","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:及时诊断和治疗炎症性肠病(IBD)可改善临床疗效:及时诊断和治疗炎症性肠病(IBD)可改善临床预后:研究 IBD 诊断时间、先前医疗保健使用模式和临床结果之间的关联:通过临床实践研究数据链,我们确定了 2003 年 1 月至 2016 年 5 月间确诊的克罗恩病(CD)和溃疡性结肠炎(UC)病例,这些病例在确诊 IBD 之前的 3 年内接受过首次初级保健胃肠道咨询。我们使用多变量考克斯回归法研究了基层医疗机构就诊频率(n=1、2、>2)、年度就诊强度、因胃肠道症状而住院治疗以及确诊时间与确诊后一系列关键临床结果之间的关系:我们发现了 2645 例 IBD 病例(CD:782 例;UC:1863 例)。就 CD 而言,>2 次就诊与肠道手术(调整 HR (aHR)=2.22, 95% CI 1.45 至 3.39)和随后与 CD 相关的住院治疗(aHR=1.80, 95% CI 1.29 至 2.50)有关。对于 UC,超过 2 次就诊与皮质类固醇依赖(aHR=1.76,95% CI 1.28 至 2.41)、免疫调节剂使用(aHR=1.68,95% CI 1.24 至 2.26)、UC 相关住院(aHR=1.43,95% CI 1.05 至 1.95)和结肠切除术(aHR=2.01,95% CI 1.22 至 3.27)相关。对于 CD,诊断前住院与 CD 相关住院(aHR=1.30,95% CI 1.01 至 1.68)和肠道手术(aHR=1.71,95% CI 1.13 至 2.58)相关;对于 UC,诊断前住院与使用免疫调节剂(aHR=1.42,95% CI 1.11 至 1.81)、UC 相关住院(aHR=1.36,95% CI 1.06 至 1.95)和结肠切除术(aHR=1.54,95% CI 1.01 至 2.34)相关。对于 CD,诊断前一年的就诊强度与 CD 相关住院(aHR=1.19,95% CI 1.12 至 1.28)和肠道手术(aHR=1.13,95% CI 1.03 至 1.23)相关;对于 UC,诊断前一年的就诊强度与 UC 相关住院(aHR=1.19,95% CI 1.06 至 1.95)和结肠手术(aHR=1.54,95% CI 1.01 至 2.34)相关。23);对于 UC,它与皮质类固醇的使用(aHR=1.08,95% CI 1.04 至 1.13)、皮质类固醇依赖(aHR=1.05,95% CI 1.00 至 1.11)和 UC 相关住院(aHR=1.12,95% CI 1.03 至 1.21)有关。对于 CD,诊断时间与 CD 相关住院风险相关(aHR=1.03,95% CI 1.01 至 1.68);对于 UC,诊断时间与 UC 相关住院风险降低相关(aHR=0.83,95% CI 0.70 至 0.98),与结肠切除术相关(aHR=0.59,95% CI 0.43 至 0.80):电子病历包含有关医疗保健使用模式的宝贵信息,可用于加快及时诊断和识别侵袭性 IBD。
Associations between prior healthcare use, time to diagnosis, and clinical outcomes in inflammatory bowel disease: a nationally representative population-based cohort study.
Background: Timely diagnosis and treatment of inflammatory bowel disease (IBD) may improve clinical outcomes.
Objective: Examine associations between time to diagnosis, patterns of prior healthcare use, and clinical outcomes in IBD.
Design: Using the Clinical Practice Research Datalink we identified incident cases of Crohn's disease (CD) and ulcerative colitis (UC), diagnosed between January 2003 and May 2016, with a first primary care gastrointestinal consultation during the 3-year period prior to IBD diagnosis. We used multivariable Cox regression to examine the association of primary care consultation frequency (n=1, 2, >2), annual consultation intensity, hospitalisations for gastrointestinal symptoms, and time to diagnosis with a range of key clinical outcomes following diagnosis.
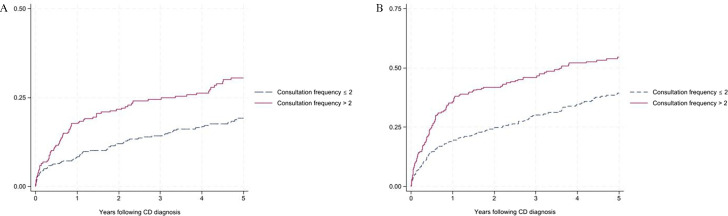
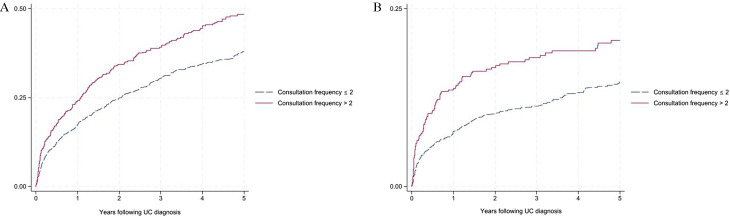
Results: We identified 2645 incident IBD cases (CD: 782; UC: 1863). For CD, >2 consultations were associated with intestinal surgery (adjusted HR (aHR)=2.22, 95% CI 1.45 to 3.39) and subsequent CD-related hospitalisation (aHR=1.80, 95% CI 1.29 to 2.50). For UC, >2 consultations were associated with corticosteroid dependency (aHR=1.76, 95% CI 1.28 to 2.41), immunomodulator use (aHR=1.68, 95% CI 1.24 to 2.26), UC-related hospitalisation (aHR=1.43, 95% CI 1.05 to 1.95) and colectomy (aHR=2.01, 95% CI 1.22 to 3.27). For CD, hospitalisation prior to diagnosis was associated with CD-related hospitalisation (aHR=1.30, 95% CI 1.01 to 1.68) and intestinal surgery (aHR=1.71, 95% CI 1.13 to 2.58); for UC, it was associated with immunomodulator use (aHR=1.42, 95% CI 1.11 to 1.81), UC-related hospitalisation (aHR=1.36, 95% CI 1.06 to 1.95) and colectomy (aHR=1.54, 95% CI 1.01 to 2.34). For CD, consultation intensity in the year before diagnosis was associated with CD-related hospitalisation (aHR=1.19, 95% CI 1.12 to 1.28) and intestinal surgery (aHR=1.13, 95% CI 1.03 to 1.23); for UC, it was associated with corticosteroid use (aHR=1.08, 95% CI 1.04 to 1.13), corticosteroid dependency (aHR=1.05, 95% CI 1.00 to 1.11), and UC-related hospitalisation (aHR=1.12, 95% CI 1.03 to 1.21). For CD, time to diagnosis was associated with risk of CD-related hospitalisation (aHR=1.03, 95% CI 1.01 to 1.68); for UC, it was associated with reduced risk of UC-related hospitalisation (aHR=0.83, 95% CI 0.70 to 0.98) and colectomy (aHR=0.59, 95% CI 0.43 to 0.80).
Conclusion: Electronic records contain valuable information about patterns of healthcare use that can be used to expedite timely diagnosis and identify aggressive forms of IBD.
期刊介绍:
BMJ Open Gastroenterology is an online-only, peer-reviewed, open access gastroenterology journal, dedicated to publishing high-quality medical research from all disciplines and therapeutic areas of gastroenterology. It is the open access companion journal of Gut and is co-owned by the British Society of Gastroenterology. The journal publishes all research study types, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Publishing procedures are built around continuous publication, publishing research online as soon as the article is ready.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
