{"title":"复发性非动脉炎性视网膜动脉闭塞的临床特征。","authors":"Hyeong Min Kim, Se Joon Woo","doi":"10.1136/bmjophth-2024-001636","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the recurrent non-arteritic retinal artery occlusion (RAO) in the same or opposite eye.</p><p><strong>Methods: </strong>We searched the RAO registry at Seoul National University Bundang Hospital and included patients with recurrent RAO in the present study. Ophthalmic and systemic features were analysed to identify risk factors and visual outcomes.</p><p><strong>Results: </strong>Of the 850 patients in the non-arteritic RAO cohort, 11 (1.3%) experienced a second RAO recurrence, either in the same (5 patients; 0.6%) or opposite (6 patients; 0.7%) eye. The same eye group experienced an earlier recurrence (1-2 months, median 1 month) than the opposite eye group, where the time to recurrence was notably longer (8-66 months, median 22 months). Best corrected visual acuity (BCVA) in the same eye group decreased after the recurrence of RAO. In the same eye group, initial BCVA ranged from 20/200 to counting fingers (CF), while BCVA during RAO recurrence ranged from CF to hand motion. When RAO recurred in the opposite eye, the reduction in visual acuity was less severe than the reduction of the initial episode: initial episode ranged from 20/400 to light perception and recurrent episode ranged from 20/25 to 20/400. Patients exhibited varying degrees of carotid (81.8%) and cerebral (9.1%) artery occlusions. Additionally, one patient in each group (total 2 patients, 18.2%) experienced a stroke 6 months after RAO recurrence.</p><p><strong>Conclusions: </strong>Since the RAO recurrences could lead to devastating visual impairment, it is essential to emphasise the importance of risk factor screening to patients while collaborating with neurologists and cardiologists.</p>","PeriodicalId":9286,"journal":{"name":"BMJ Open Ophthalmology","volume":"9 1","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2024-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11138310/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical characteristics of recurrent non-arteritic retinal artery occlusion.\",\"authors\":\"Hyeong Min Kim, Se Joon Woo\",\"doi\":\"10.1136/bmjophth-2024-001636\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To investigate the recurrent non-arteritic retinal artery occlusion (RAO) in the same or opposite eye.</p><p><strong>Methods: </strong>We searched the RAO registry at Seoul National University Bundang Hospital and included patients with recurrent RAO in the present study. Ophthalmic and systemic features were analysed to identify risk factors and visual outcomes.</p><p><strong>Results: </strong>Of the 850 patients in the non-arteritic RAO cohort, 11 (1.3%) experienced a second RAO recurrence, either in the same (5 patients; 0.6%) or opposite (6 patients; 0.7%) eye. The same eye group experienced an earlier recurrence (1-2 months, median 1 month) than the opposite eye group, where the time to recurrence was notably longer (8-66 months, median 22 months). Best corrected visual acuity (BCVA) in the same eye group decreased after the recurrence of RAO. In the same eye group, initial BCVA ranged from 20/200 to counting fingers (CF), while BCVA during RAO recurrence ranged from CF to hand motion. When RAO recurred in the opposite eye, the reduction in visual acuity was less severe than the reduction of the initial episode: initial episode ranged from 20/400 to light perception and recurrent episode ranged from 20/25 to 20/400. Patients exhibited varying degrees of carotid (81.8%) and cerebral (9.1%) artery occlusions. Additionally, one patient in each group (total 2 patients, 18.2%) experienced a stroke 6 months after RAO recurrence.</p><p><strong>Conclusions: </strong>Since the RAO recurrences could lead to devastating visual impairment, it is essential to emphasise the importance of risk factor screening to patients while collaborating with neurologists and cardiologists.</p>\",\"PeriodicalId\":9286,\"journal\":{\"name\":\"BMJ Open Ophthalmology\",\"volume\":\"9 1\",\"pages\":\"\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11138310/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Ophthalmology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjophth-2024-001636\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"OPHTHALMOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjophth-2024-001636","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
Clinical characteristics of recurrent non-arteritic retinal artery occlusion.
Objectives: To investigate the recurrent non-arteritic retinal artery occlusion (RAO) in the same or opposite eye.
Methods: We searched the RAO registry at Seoul National University Bundang Hospital and included patients with recurrent RAO in the present study. Ophthalmic and systemic features were analysed to identify risk factors and visual outcomes.
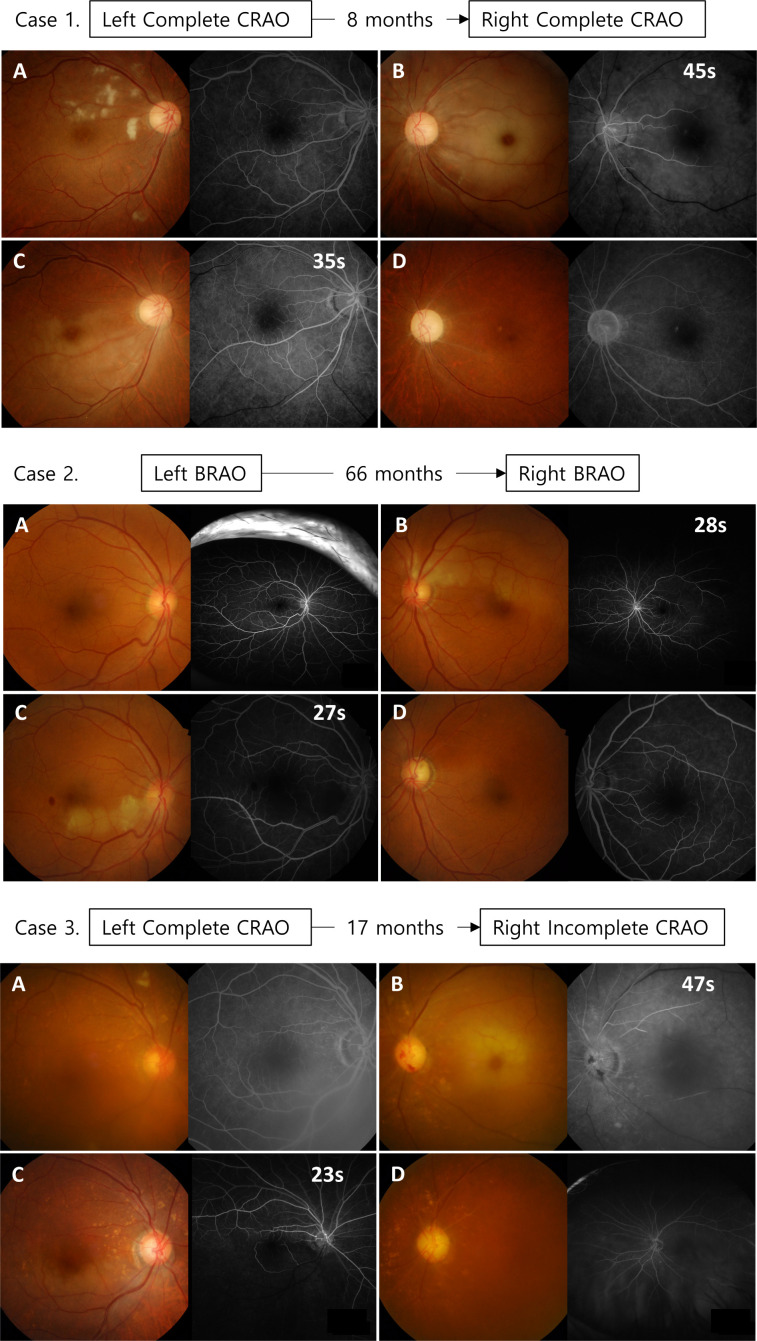
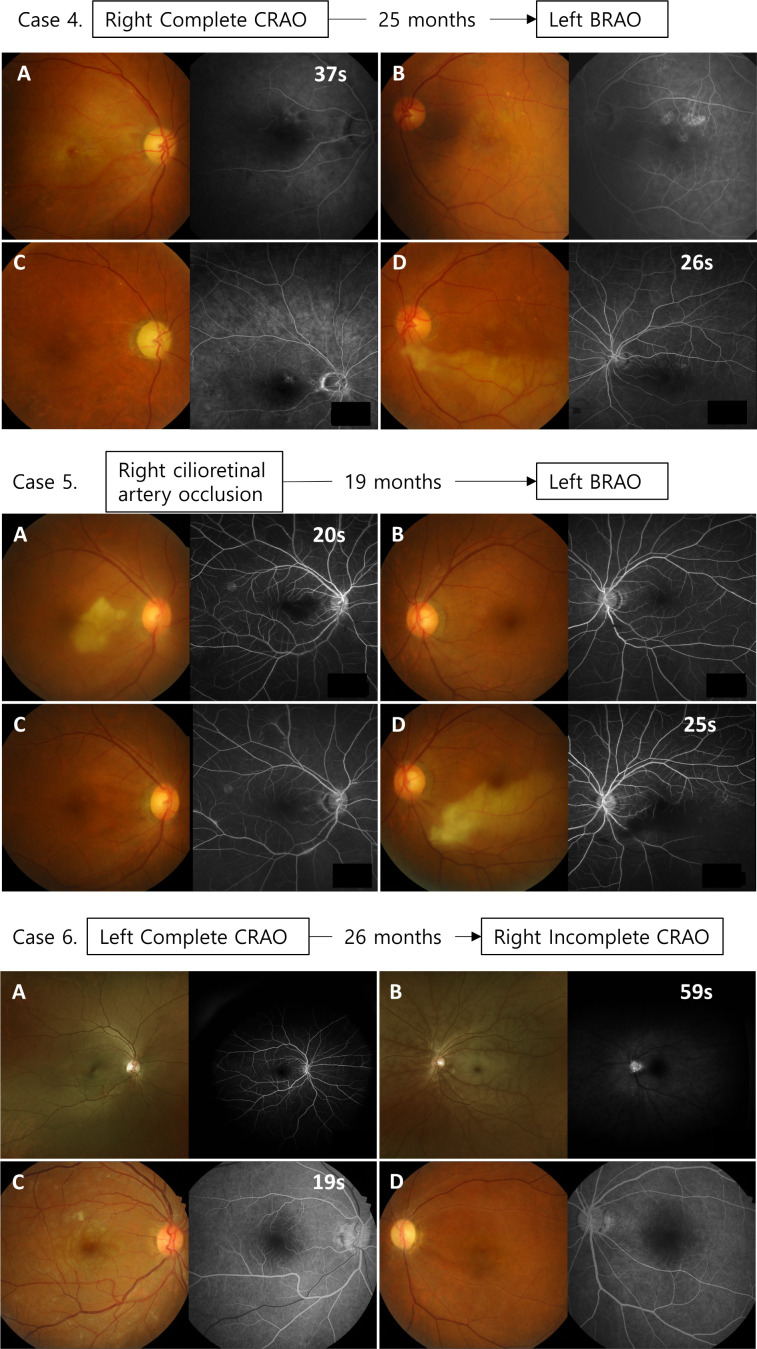
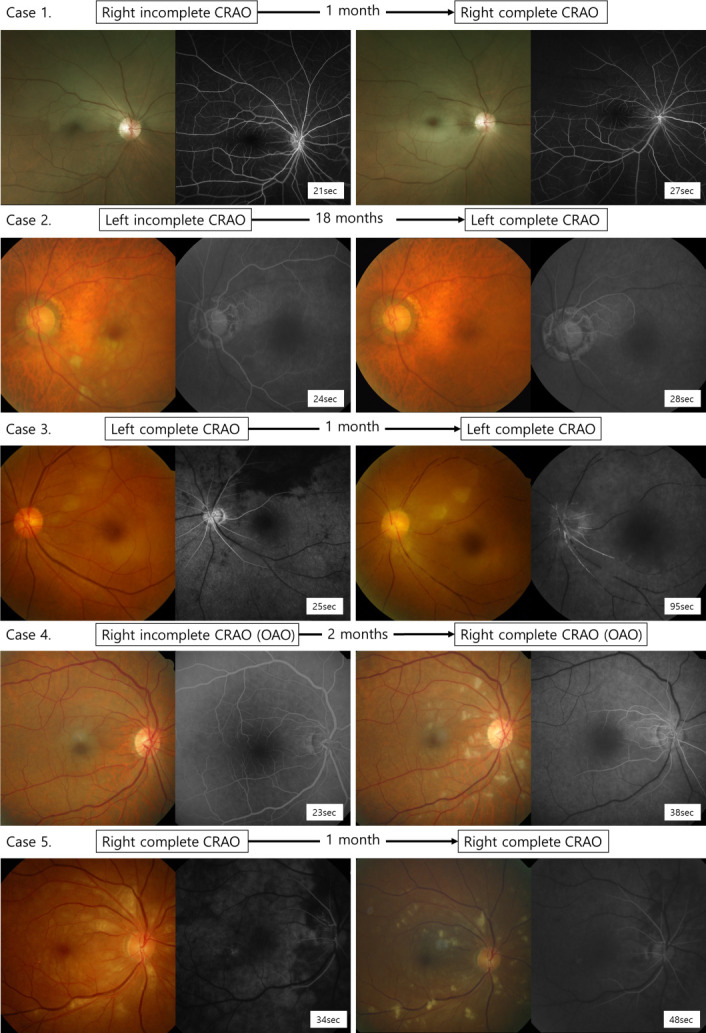
Results: Of the 850 patients in the non-arteritic RAO cohort, 11 (1.3%) experienced a second RAO recurrence, either in the same (5 patients; 0.6%) or opposite (6 patients; 0.7%) eye. The same eye group experienced an earlier recurrence (1-2 months, median 1 month) than the opposite eye group, where the time to recurrence was notably longer (8-66 months, median 22 months). Best corrected visual acuity (BCVA) in the same eye group decreased after the recurrence of RAO. In the same eye group, initial BCVA ranged from 20/200 to counting fingers (CF), while BCVA during RAO recurrence ranged from CF to hand motion. When RAO recurred in the opposite eye, the reduction in visual acuity was less severe than the reduction of the initial episode: initial episode ranged from 20/400 to light perception and recurrent episode ranged from 20/25 to 20/400. Patients exhibited varying degrees of carotid (81.8%) and cerebral (9.1%) artery occlusions. Additionally, one patient in each group (total 2 patients, 18.2%) experienced a stroke 6 months after RAO recurrence.
Conclusions: Since the RAO recurrences could lead to devastating visual impairment, it is essential to emphasise the importance of risk factor screening to patients while collaborating with neurologists and cardiologists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
