Maria Molina, Mario Fernández-Ruiz, Esther Gonzalez, Jimena Cabrera, Manuel Praga, Alfredo Rodriguez, Angel Tejido-Sánchez, Jose Medina-Polo, Alonso Mateos, Carlos Rubio-Chacón, Angel Sanchez, Ana Pla, Amado Andrés
{"title":"预防性抗凝治疗可降低肾脏阻力指数高的循环死亡捐献者在无控制捐献后接受肾脏移植物静脉血栓形成的风险。","authors":"Maria Molina, Mario Fernández-Ruiz, Esther Gonzalez, Jimena Cabrera, Manuel Praga, Alfredo Rodriguez, Angel Tejido-Sánchez, Jose Medina-Polo, Alonso Mateos, Carlos Rubio-Chacón, Angel Sanchez, Ana Pla, Amado Andrés","doi":"10.1097/TXD.0000000000001649","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Uncontrolled donation after circulatory death (uDCD) increases organ availability for kidney transplantation (KT) at the expense of a higher risk of primary graft nonfunction (PNF). At least half of the cases of PNF are secondary to graft venous thrombosis. The potential benefit from prophylactic anticoagulation in this scenario remains unclear.</p><p><strong>Methods: </strong>In this single-center retrospective study we compared 2 consecutive cohorts of KT from uDCD with increased (≥0.8) renal resistive index (RRI) in the Doppler ultrasound examination performed within the first 24-72 h after transplantation: 36 patients did not receive anticoagulation (\"nonanticoagulation group\") and 71 patients underwent prophylactic anticoagulation until normalization of RRI in follow-up Doppler examinations (\"anticoagulation group\").</p><p><strong>Results: </strong>Anticoagulation was initiated at a median of 2 d (interquartile range, 2-3) after transplantation and maintained for a median of 12 d (interquartile range, 7-18). In 4 patients (5.6%), anticoagulation had to be prematurely stopped because of the development of a hemorrhagic complication. In comparison with the nonanticoagulation group, recipients in the anticoagulation group had a lower 2-wk cumulative incidence of graft venous thrombosis (19.4% versus 0.0%; <i>P</i> < 0.001) and PNF (19.4% versus 2.8%; <i>P</i> = 0.006). The competing risk analysis with nonthrombotic causes of PNF as the competitive event confirmed the higher risk of graft thrombosis in the nonanticoagulation group <i>(P</i> = 0.0001). The anticoagulation group had a higher incidence of macroscopic hematuria (21.1% versus 5.6%; <i>P</i> = 0.049) and blood transfusion requirements (39.4% versus 19.4%; <i>P</i> = 0.050) compared with the nonanticoagulation group. No graft losses or deaths were attributable to complications potentially associated with anticoagulation.</p><p><strong>Conclusions: </strong>Early initiation of prophylactic anticoagulation in selected KT recipients from uDCD with an early Doppler ultrasound RRI of ≥0.8 within the first 24-72 h may reduce the incidence of graft venous thrombosis as a cause of PNF.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 6","pages":"e1649"},"PeriodicalIF":1.9000,"publicationDate":"2024-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11139466/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prophylactic Anticoagulation Reduces the Risk of Kidney Graft Venous Thrombosis in Recipients From Uncontrolled Donation After Circulatory Death Donors With High Renal Resistive Index.\",\"authors\":\"Maria Molina, Mario Fernández-Ruiz, Esther Gonzalez, Jimena Cabrera, Manuel Praga, Alfredo Rodriguez, Angel Tejido-Sánchez, Jose Medina-Polo, Alonso Mateos, Carlos Rubio-Chacón, Angel Sanchez, Ana Pla, Amado Andrés\",\"doi\":\"10.1097/TXD.0000000000001649\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Uncontrolled donation after circulatory death (uDCD) increases organ availability for kidney transplantation (KT) at the expense of a higher risk of primary graft nonfunction (PNF). At least half of the cases of PNF are secondary to graft venous thrombosis. The potential benefit from prophylactic anticoagulation in this scenario remains unclear.</p><p><strong>Methods: </strong>In this single-center retrospective study we compared 2 consecutive cohorts of KT from uDCD with increased (≥0.8) renal resistive index (RRI) in the Doppler ultrasound examination performed within the first 24-72 h after transplantation: 36 patients did not receive anticoagulation (\\\"nonanticoagulation group\\\") and 71 patients underwent prophylactic anticoagulation until normalization of RRI in follow-up Doppler examinations (\\\"anticoagulation group\\\").</p><p><strong>Results: </strong>Anticoagulation was initiated at a median of 2 d (interquartile range, 2-3) after transplantation and maintained for a median of 12 d (interquartile range, 7-18). In 4 patients (5.6%), anticoagulation had to be prematurely stopped because of the development of a hemorrhagic complication. In comparison with the nonanticoagulation group, recipients in the anticoagulation group had a lower 2-wk cumulative incidence of graft venous thrombosis (19.4% versus 0.0%; <i>P</i> < 0.001) and PNF (19.4% versus 2.8%; <i>P</i> = 0.006). The competing risk analysis with nonthrombotic causes of PNF as the competitive event confirmed the higher risk of graft thrombosis in the nonanticoagulation group <i>(P</i> = 0.0001). The anticoagulation group had a higher incidence of macroscopic hematuria (21.1% versus 5.6%; <i>P</i> = 0.049) and blood transfusion requirements (39.4% versus 19.4%; <i>P</i> = 0.050) compared with the nonanticoagulation group. No graft losses or deaths were attributable to complications potentially associated with anticoagulation.</p><p><strong>Conclusions: </strong>Early initiation of prophylactic anticoagulation in selected KT recipients from uDCD with an early Doppler ultrasound RRI of ≥0.8 within the first 24-72 h may reduce the incidence of graft venous thrombosis as a cause of PNF.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"10 6\",\"pages\":\"e1649\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-05-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11139466/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001649\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001649","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
Prophylactic Anticoagulation Reduces the Risk of Kidney Graft Venous Thrombosis in Recipients From Uncontrolled Donation After Circulatory Death Donors With High Renal Resistive Index.
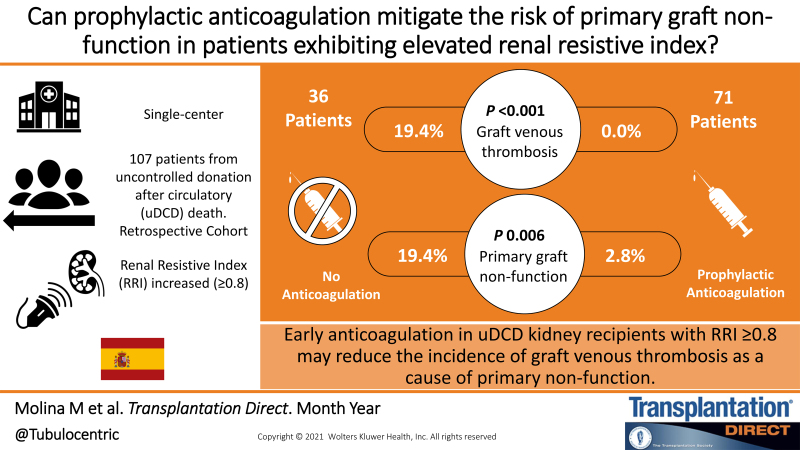
Background: Uncontrolled donation after circulatory death (uDCD) increases organ availability for kidney transplantation (KT) at the expense of a higher risk of primary graft nonfunction (PNF). At least half of the cases of PNF are secondary to graft venous thrombosis. The potential benefit from prophylactic anticoagulation in this scenario remains unclear.
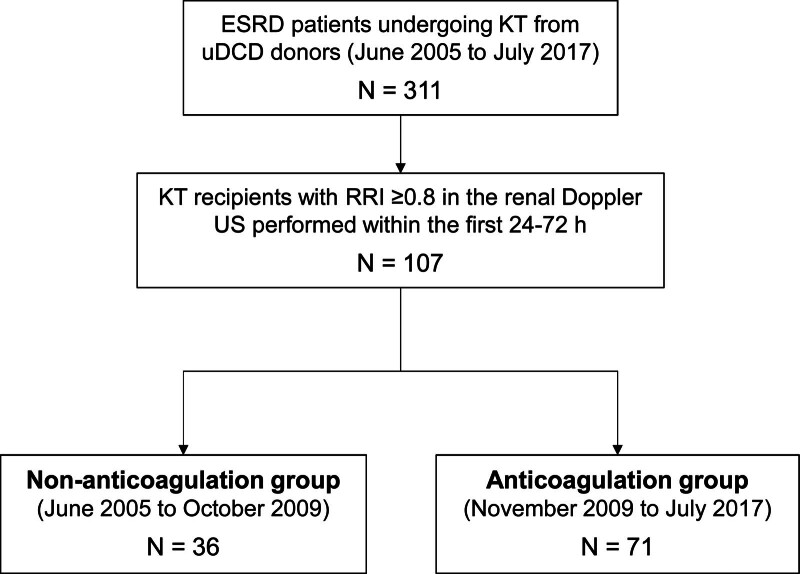
Methods: In this single-center retrospective study we compared 2 consecutive cohorts of KT from uDCD with increased (≥0.8) renal resistive index (RRI) in the Doppler ultrasound examination performed within the first 24-72 h after transplantation: 36 patients did not receive anticoagulation ("nonanticoagulation group") and 71 patients underwent prophylactic anticoagulation until normalization of RRI in follow-up Doppler examinations ("anticoagulation group").
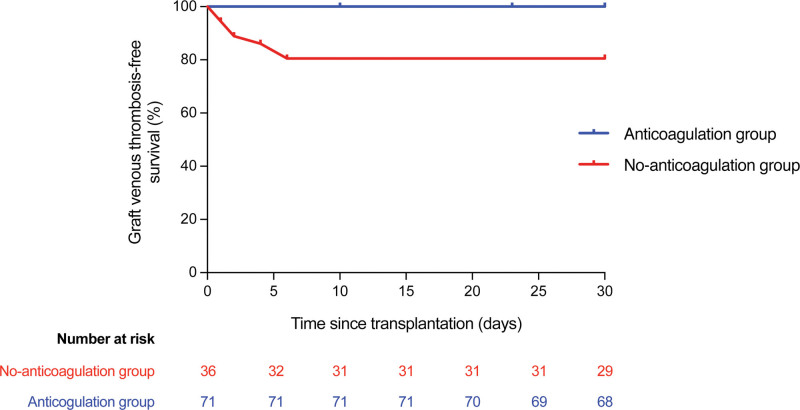
Results: Anticoagulation was initiated at a median of 2 d (interquartile range, 2-3) after transplantation and maintained for a median of 12 d (interquartile range, 7-18). In 4 patients (5.6%), anticoagulation had to be prematurely stopped because of the development of a hemorrhagic complication. In comparison with the nonanticoagulation group, recipients in the anticoagulation group had a lower 2-wk cumulative incidence of graft venous thrombosis (19.4% versus 0.0%; P < 0.001) and PNF (19.4% versus 2.8%; P = 0.006). The competing risk analysis with nonthrombotic causes of PNF as the competitive event confirmed the higher risk of graft thrombosis in the nonanticoagulation group (P = 0.0001). The anticoagulation group had a higher incidence of macroscopic hematuria (21.1% versus 5.6%; P = 0.049) and blood transfusion requirements (39.4% versus 19.4%; P = 0.050) compared with the nonanticoagulation group. No graft losses or deaths were attributable to complications potentially associated with anticoagulation.
Conclusions: Early initiation of prophylactic anticoagulation in selected KT recipients from uDCD with an early Doppler ultrasound RRI of ≥0.8 within the first 24-72 h may reduce the incidence of graft venous thrombosis as a cause of PNF.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
