Benedikt Treml, Christine Eckhardt, Christoph Oberleitner, Thomas Ploner, Christopher Rugg, Aleksandra Radovanovic Spurnic, Sasa Rajsic
{"title":"[院内心脏骤停后的生活质量:一所大学中心 11 年的经验]。","authors":"Benedikt Treml, Christine Eckhardt, Christoph Oberleitner, Thomas Ploner, Christopher Rugg, Aleksandra Radovanovic Spurnic, Sasa Rajsic","doi":"10.1007/s00101-024-01423-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac arrest is a life-threatening condition requiring urgent medical care and is one of the leading causes of death worldwide. Given that in-hospital cardiac arrest (IHCA) is still poorly investigated, data on health-associated quality of life thereafter remains scarce. The available evidence is mostly transferred from out-of-hospital cardiac arrest studies, but the epidemiology and determinants of success might be different. The aim of the study was to investigate the change in the quality of life after in-hospital cardiac arrest and to identify potential risk factors for a poor outcome.</p><p><strong>Material and methods: </strong>This retrospective analysis of data and prospective evaluation of quality of life included all patients surviving an IHCA and being treated by the emergency medical team between 2010 and 2020. The primary endpoint of the study was the quality of life after IHCA at the reference date. Secondary endpoints covered determination of risk factors and predictors of poor outcome after in-hospital cardiopulmonary resuscitation.</p><p><strong>Results: </strong>In total 604 patients were resuscitated within the period of 11 years and 61 (10%) patients survived until the interview took place. Finally, 48 (79%) patients fulfilled the inclusion criteria and 31 (65%) were included in the study. There was no significant difference in the quality of life before and after cardiac arrest (EQ-5D-5L utility 0.79 vs. 0.78, p = 0.567) and in the EQ-5D-5L visual analogue scale (VAS) score.</p><p><strong>Conclusion: </strong>The quality of life before and after IHCA in survivors was good and comparable. The quality of life was mostly affected by reduced mobility and anxiety/depression. Future studies with larger patient samples should focus on potentially modifiable factors that could prevent, warn, and limit the consequences of in-hospital cardiac arrest. Moreover, research on outcomes of IHCA should include available tools for the quality of life assessment.</p>","PeriodicalId":72805,"journal":{"name":"Die Anaesthesiologie","volume":" ","pages":"454-461"},"PeriodicalIF":1.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11222208/pdf/","citationCount":"0","resultStr":"{\"title\":\"[Quality of life after in-hospital cardiac arrest : An 11-year experience from an university center].\",\"authors\":\"Benedikt Treml, Christine Eckhardt, Christoph Oberleitner, Thomas Ploner, Christopher Rugg, Aleksandra Radovanovic Spurnic, Sasa Rajsic\",\"doi\":\"10.1007/s00101-024-01423-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiac arrest is a life-threatening condition requiring urgent medical care and is one of the leading causes of death worldwide. Given that in-hospital cardiac arrest (IHCA) is still poorly investigated, data on health-associated quality of life thereafter remains scarce. The available evidence is mostly transferred from out-of-hospital cardiac arrest studies, but the epidemiology and determinants of success might be different. The aim of the study was to investigate the change in the quality of life after in-hospital cardiac arrest and to identify potential risk factors for a poor outcome.</p><p><strong>Material and methods: </strong>This retrospective analysis of data and prospective evaluation of quality of life included all patients surviving an IHCA and being treated by the emergency medical team between 2010 and 2020. The primary endpoint of the study was the quality of life after IHCA at the reference date. Secondary endpoints covered determination of risk factors and predictors of poor outcome after in-hospital cardiopulmonary resuscitation.</p><p><strong>Results: </strong>In total 604 patients were resuscitated within the period of 11 years and 61 (10%) patients survived until the interview took place. Finally, 48 (79%) patients fulfilled the inclusion criteria and 31 (65%) were included in the study. There was no significant difference in the quality of life before and after cardiac arrest (EQ-5D-5L utility 0.79 vs. 0.78, p = 0.567) and in the EQ-5D-5L visual analogue scale (VAS) score.</p><p><strong>Conclusion: </strong>The quality of life before and after IHCA in survivors was good and comparable. The quality of life was mostly affected by reduced mobility and anxiety/depression. Future studies with larger patient samples should focus on potentially modifiable factors that could prevent, warn, and limit the consequences of in-hospital cardiac arrest. Moreover, research on outcomes of IHCA should include available tools for the quality of life assessment.</p>\",\"PeriodicalId\":72805,\"journal\":{\"name\":\"Die Anaesthesiologie\",\"volume\":\" \",\"pages\":\"454-461\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11222208/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Die Anaesthesiologie\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s00101-024-01423-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Die Anaesthesiologie","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00101-024-01423-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
[Quality of life after in-hospital cardiac arrest : An 11-year experience from an university center].
Background: Cardiac arrest is a life-threatening condition requiring urgent medical care and is one of the leading causes of death worldwide. Given that in-hospital cardiac arrest (IHCA) is still poorly investigated, data on health-associated quality of life thereafter remains scarce. The available evidence is mostly transferred from out-of-hospital cardiac arrest studies, but the epidemiology and determinants of success might be different. The aim of the study was to investigate the change in the quality of life after in-hospital cardiac arrest and to identify potential risk factors for a poor outcome.
Material and methods: This retrospective analysis of data and prospective evaluation of quality of life included all patients surviving an IHCA and being treated by the emergency medical team between 2010 and 2020. The primary endpoint of the study was the quality of life after IHCA at the reference date. Secondary endpoints covered determination of risk factors and predictors of poor outcome after in-hospital cardiopulmonary resuscitation.
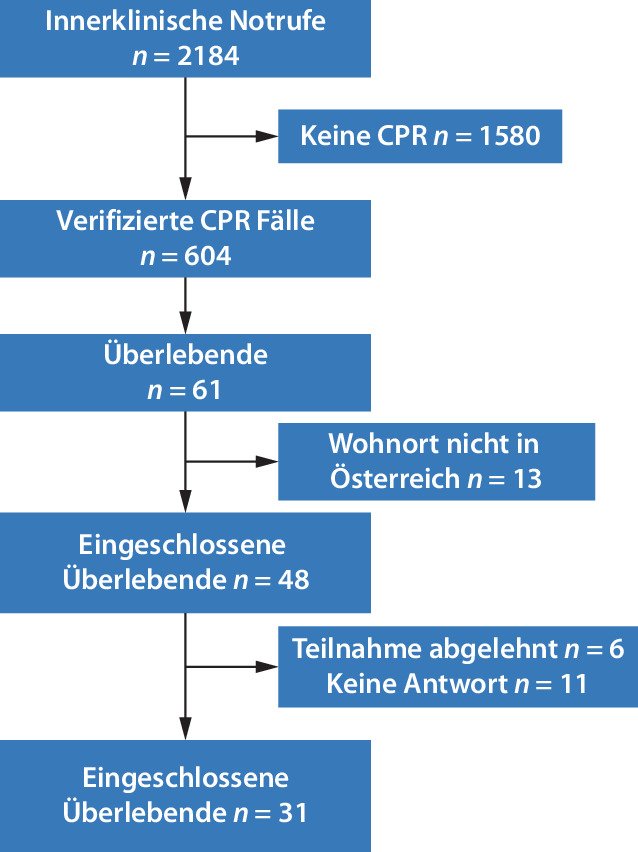
Results: In total 604 patients were resuscitated within the period of 11 years and 61 (10%) patients survived until the interview took place. Finally, 48 (79%) patients fulfilled the inclusion criteria and 31 (65%) were included in the study. There was no significant difference in the quality of life before and after cardiac arrest (EQ-5D-5L utility 0.79 vs. 0.78, p = 0.567) and in the EQ-5D-5L visual analogue scale (VAS) score.
Conclusion: The quality of life before and after IHCA in survivors was good and comparable. The quality of life was mostly affected by reduced mobility and anxiety/depression. Future studies with larger patient samples should focus on potentially modifiable factors that could prevent, warn, and limit the consequences of in-hospital cardiac arrest. Moreover, research on outcomes of IHCA should include available tools for the quality of life assessment.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
