Hossameldin Rezk, Ghada Youssef, Karim Said, Iman Mandour, Magdy Abdelhamid
{"title":"腹部充血是急性失代偿性心力衰竭患者肾功能恶化的预兆。","authors":"Hossameldin Rezk, Ghada Youssef, Karim Said, Iman Mandour, Magdy Abdelhamid","doi":"10.37616/2212-5043.1371","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Worsening renal function is a frequent finding in patients with acute decompensated heart failure (ADHF) and is a powerful independent prognostic factor for adverse outcomes. The link between abdominal congestion and worsening renal function in such patients is not yet fully addressed.</p><p><strong>Objective: </strong>To evaluate the role of abdominal congestion in the early prediction of worsening renal function in hospitalized patients with acute decompensated heart failure.</p><p><strong>Methods: </strong>This was a prospective study that enrolled 100 patients with a diagnosis of ADHF and received intravenous diuretic therapy. Intra-abdominal pressure (IAP), splenic Doppler impedance indices and serum prouroguanylin were measured on admission, 24 h after admission and on discharge. Patients were then divided into 2 groups: those who developed WRF (WRF group), and those who did not (non-WRF group). Worsening renal function was defined as an increase in serum creatinine level ≥0.3 mg/dL above baseline admission value. Intrabdominal pressure was measured transvesically using standard Foley catheter. Splenic Doppler impedance indices (resistivity and pulsatility indices) were measured using splenic Doppler ultrasound.</p><p><strong>Results: </strong>Among recruited patients (age: 54.73 ± 13.1 years, 72% are male), there was a significant decline in IAP (6.67 mmHg vs 8.36 mmHg, p = 0.001) and significant rise in splenic resistivity index (0.69 vs 0.67, p = 0.002) before discharge compared to admission values. The median level of serum prouroguanylin before discharge showed significant decline compared to admission level (29.2 vs 34.6 ng/l, p = 0.006). WRF developed in 37 (37%) patients. Independent predictors of WRF during hospitalization were high splenic arterial resistivity index 24 h after admission, high intra-abdominal pressure (≥8 mmHg) 24 h after admission, and low LVEF on admission.</p><p><strong>Conclusion: </strong>In ADHF patients receiving diuretic therapy, transvesical measurement of intra-abdominal pressure and splenic resistivity index by splenic Doppler early after admission can help to identify patients at increased risk of WRF near discharge.</p>","PeriodicalId":17319,"journal":{"name":"Journal of the Saudi Heart Association","volume":"36 1","pages":"60-69"},"PeriodicalIF":1.4000,"publicationDate":"2024-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11146666/pdf/","citationCount":"0","resultStr":"{\"title\":\"Abdominal Congestion as a Predictor of Worsening Renal Function in Patients With Acute Decompensated Heart Failure.\",\"authors\":\"Hossameldin Rezk, Ghada Youssef, Karim Said, Iman Mandour, Magdy Abdelhamid\",\"doi\":\"10.37616/2212-5043.1371\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Worsening renal function is a frequent finding in patients with acute decompensated heart failure (ADHF) and is a powerful independent prognostic factor for adverse outcomes. The link between abdominal congestion and worsening renal function in such patients is not yet fully addressed.</p><p><strong>Objective: </strong>To evaluate the role of abdominal congestion in the early prediction of worsening renal function in hospitalized patients with acute decompensated heart failure.</p><p><strong>Methods: </strong>This was a prospective study that enrolled 100 patients with a diagnosis of ADHF and received intravenous diuretic therapy. Intra-abdominal pressure (IAP), splenic Doppler impedance indices and serum prouroguanylin were measured on admission, 24 h after admission and on discharge. Patients were then divided into 2 groups: those who developed WRF (WRF group), and those who did not (non-WRF group). Worsening renal function was defined as an increase in serum creatinine level ≥0.3 mg/dL above baseline admission value. Intrabdominal pressure was measured transvesically using standard Foley catheter. Splenic Doppler impedance indices (resistivity and pulsatility indices) were measured using splenic Doppler ultrasound.</p><p><strong>Results: </strong>Among recruited patients (age: 54.73 ± 13.1 years, 72% are male), there was a significant decline in IAP (6.67 mmHg vs 8.36 mmHg, p = 0.001) and significant rise in splenic resistivity index (0.69 vs 0.67, p = 0.002) before discharge compared to admission values. The median level of serum prouroguanylin before discharge showed significant decline compared to admission level (29.2 vs 34.6 ng/l, p = 0.006). WRF developed in 37 (37%) patients. Independent predictors of WRF during hospitalization were high splenic arterial resistivity index 24 h after admission, high intra-abdominal pressure (≥8 mmHg) 24 h after admission, and low LVEF on admission.</p><p><strong>Conclusion: </strong>In ADHF patients receiving diuretic therapy, transvesical measurement of intra-abdominal pressure and splenic resistivity index by splenic Doppler early after admission can help to identify patients at increased risk of WRF near discharge.</p>\",\"PeriodicalId\":17319,\"journal\":{\"name\":\"Journal of the Saudi Heart Association\",\"volume\":\"36 1\",\"pages\":\"60-69\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-05-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11146666/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Saudi Heart Association\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.37616/2212-5043.1371\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Saudi Heart Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37616/2212-5043.1371","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Abdominal Congestion as a Predictor of Worsening Renal Function in Patients With Acute Decompensated Heart Failure.
Background: Worsening renal function is a frequent finding in patients with acute decompensated heart failure (ADHF) and is a powerful independent prognostic factor for adverse outcomes. The link between abdominal congestion and worsening renal function in such patients is not yet fully addressed.
Objective: To evaluate the role of abdominal congestion in the early prediction of worsening renal function in hospitalized patients with acute decompensated heart failure.
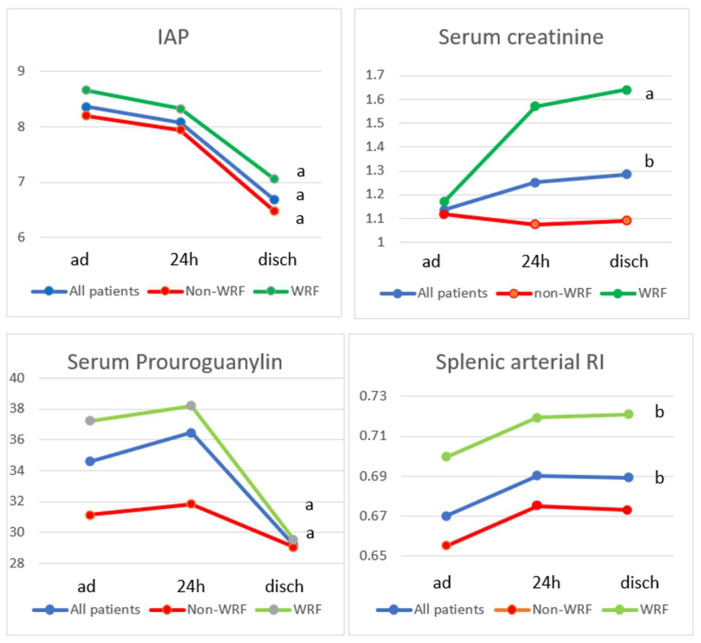
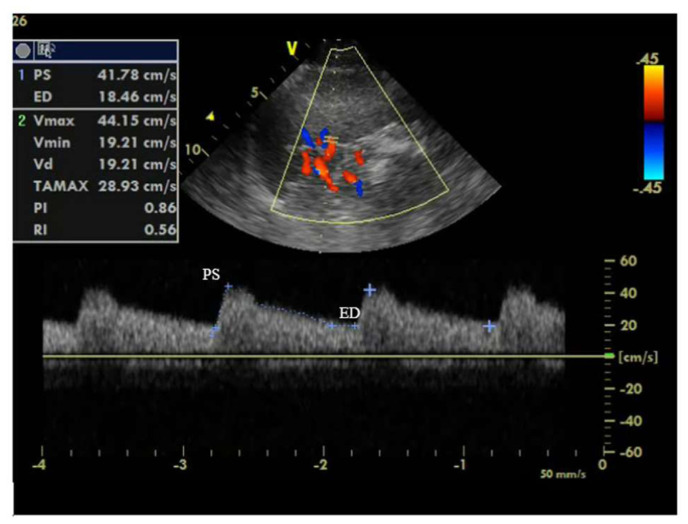
Methods: This was a prospective study that enrolled 100 patients with a diagnosis of ADHF and received intravenous diuretic therapy. Intra-abdominal pressure (IAP), splenic Doppler impedance indices and serum prouroguanylin were measured on admission, 24 h after admission and on discharge. Patients were then divided into 2 groups: those who developed WRF (WRF group), and those who did not (non-WRF group). Worsening renal function was defined as an increase in serum creatinine level ≥0.3 mg/dL above baseline admission value. Intrabdominal pressure was measured transvesically using standard Foley catheter. Splenic Doppler impedance indices (resistivity and pulsatility indices) were measured using splenic Doppler ultrasound.
Results: Among recruited patients (age: 54.73 ± 13.1 years, 72% are male), there was a significant decline in IAP (6.67 mmHg vs 8.36 mmHg, p = 0.001) and significant rise in splenic resistivity index (0.69 vs 0.67, p = 0.002) before discharge compared to admission values. The median level of serum prouroguanylin before discharge showed significant decline compared to admission level (29.2 vs 34.6 ng/l, p = 0.006). WRF developed in 37 (37%) patients. Independent predictors of WRF during hospitalization were high splenic arterial resistivity index 24 h after admission, high intra-abdominal pressure (≥8 mmHg) 24 h after admission, and low LVEF on admission.
Conclusion: In ADHF patients receiving diuretic therapy, transvesical measurement of intra-abdominal pressure and splenic resistivity index by splenic Doppler early after admission can help to identify patients at increased risk of WRF near discharge.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
