{"title":"楔形膜甲状腺癌术前诊断的困难之处","authors":"Li-Hsin Pan, Jen-Fan Hang, Jui-Yu Chen, Po-Sheng Lee, Yun-Kai Yeh, Tai-Jung Huang, Chii-Min Hwu, Chin-Sung Kuo","doi":"10.1155/2024/6517236","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cribriform morular thyroid carcinoma has been recently renamed in the 2022 WHO classification as a thyroid tumor of uncertain histogenesis. The epidemiologic, pathological, and pathophysiological characteristics distinguish it from papillary thyroid carcinoma (PTC). Preoperative genetic testing plays a role in facilitating the differential diagnosis.</p><p><strong>Methods: </strong>This report presents a confirmed case of cribriform morular thyroid carcinoma. Initially, fine-needle aspiration cytology suggested a diagnosis of PTC. However, a genetic analysis did not reveal the typical mutations associated with follicular-cell-derived neoplasms.</p><p><strong>Results: </strong>A 31-year-old woman was found to have a thyroid nodule at the left lobe measuring 11.8 × 10.2 × 12.4 mm. Ultrasonography indicated a hypoechoic, solid nodule with regular margins. Cytology revealed a papillary structure of tall cells, leading to a PTC diagnosis. Nevertheless, the genetic analysis failed to detect mutations such as <i>BRAF V600E</i>, <i>NRAS Q61R</i>, <i>NRAS Q61K</i>, <i>HRAS Q61R</i>, <i>or HRAS Q61K</i> mutation or the fusion of <i>CCDC6-RET</i>, <i>NCOA4-RET</i>, <i>PAX8-PPARG</i>, <i>ETV6-NTRK3</i>, <i>TPM3-NTRK1</i>, <i>IRF2BP2-NTRK1</i>, or <i>SQSTM1-NTRK1</i> in the aspirated follicular cells. The patient subsequently underwent total thyroidectomy with central lymph node dissection. Pathological examination revealed a cribriform pattern of spindle-shaped cells with morular areas. Immunohistochemical staining showed positive results for <i>β</i>-catenin and TTF-1, except in the morular regions, and negative results for PAX8, thyroglobulin, and BRAF (clone VE1). The diagnosis was confirmed to be cribriform morular thyroid carcinoma.</p><p><strong>Conclusion: </strong>Significant cytological similarity exists between PTC and cribriform morular thyroid carcinoma. Preoperative genetic analysis is important to differentiate these two diseases. Cribriform morular thyroid carcinoma can be differentiated from common follicular-cell-derived tumors by the absence of typical mutations; the presence of nuclear and cytoplasmic expressions of <i>β</i>-catenin; the presence of TTF-1, except in morular areas; and the absence of thyroglobulin.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2024 ","pages":"6517236"},"PeriodicalIF":0.9000,"publicationDate":"2024-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11150044/pdf/","citationCount":"0","resultStr":"{\"title\":\"Difficulties of Preoperative Diagnosis of Cribriform Morular Thyroid Carcinoma.\",\"authors\":\"Li-Hsin Pan, Jen-Fan Hang, Jui-Yu Chen, Po-Sheng Lee, Yun-Kai Yeh, Tai-Jung Huang, Chii-Min Hwu, Chin-Sung Kuo\",\"doi\":\"10.1155/2024/6517236\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cribriform morular thyroid carcinoma has been recently renamed in the 2022 WHO classification as a thyroid tumor of uncertain histogenesis. The epidemiologic, pathological, and pathophysiological characteristics distinguish it from papillary thyroid carcinoma (PTC). Preoperative genetic testing plays a role in facilitating the differential diagnosis.</p><p><strong>Methods: </strong>This report presents a confirmed case of cribriform morular thyroid carcinoma. Initially, fine-needle aspiration cytology suggested a diagnosis of PTC. However, a genetic analysis did not reveal the typical mutations associated with follicular-cell-derived neoplasms.</p><p><strong>Results: </strong>A 31-year-old woman was found to have a thyroid nodule at the left lobe measuring 11.8 × 10.2 × 12.4 mm. Ultrasonography indicated a hypoechoic, solid nodule with regular margins. Cytology revealed a papillary structure of tall cells, leading to a PTC diagnosis. Nevertheless, the genetic analysis failed to detect mutations such as <i>BRAF V600E</i>, <i>NRAS Q61R</i>, <i>NRAS Q61K</i>, <i>HRAS Q61R</i>, <i>or HRAS Q61K</i> mutation or the fusion of <i>CCDC6-RET</i>, <i>NCOA4-RET</i>, <i>PAX8-PPARG</i>, <i>ETV6-NTRK3</i>, <i>TPM3-NTRK1</i>, <i>IRF2BP2-NTRK1</i>, or <i>SQSTM1-NTRK1</i> in the aspirated follicular cells. The patient subsequently underwent total thyroidectomy with central lymph node dissection. Pathological examination revealed a cribriform pattern of spindle-shaped cells with morular areas. Immunohistochemical staining showed positive results for <i>β</i>-catenin and TTF-1, except in the morular regions, and negative results for PAX8, thyroglobulin, and BRAF (clone VE1). The diagnosis was confirmed to be cribriform morular thyroid carcinoma.</p><p><strong>Conclusion: </strong>Significant cytological similarity exists between PTC and cribriform morular thyroid carcinoma. Preoperative genetic analysis is important to differentiate these two diseases. Cribriform morular thyroid carcinoma can be differentiated from common follicular-cell-derived tumors by the absence of typical mutations; the presence of nuclear and cytoplasmic expressions of <i>β</i>-catenin; the presence of TTF-1, except in morular areas; and the absence of thyroglobulin.</p>\",\"PeriodicalId\":9621,\"journal\":{\"name\":\"Case Reports in Endocrinology\",\"volume\":\"2024 \",\"pages\":\"6517236\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-05-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11150044/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/6517236\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/6517236","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Difficulties of Preoperative Diagnosis of Cribriform Morular Thyroid Carcinoma.
Background: Cribriform morular thyroid carcinoma has been recently renamed in the 2022 WHO classification as a thyroid tumor of uncertain histogenesis. The epidemiologic, pathological, and pathophysiological characteristics distinguish it from papillary thyroid carcinoma (PTC). Preoperative genetic testing plays a role in facilitating the differential diagnosis.
Methods: This report presents a confirmed case of cribriform morular thyroid carcinoma. Initially, fine-needle aspiration cytology suggested a diagnosis of PTC. However, a genetic analysis did not reveal the typical mutations associated with follicular-cell-derived neoplasms.
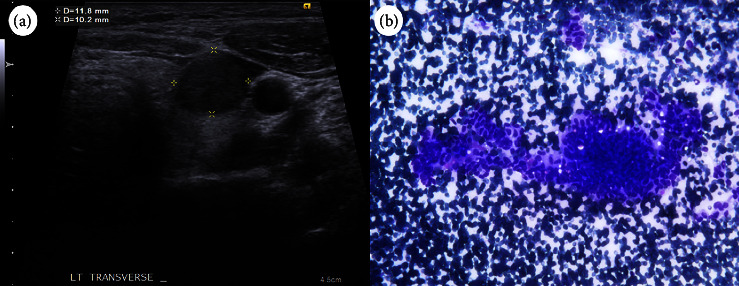
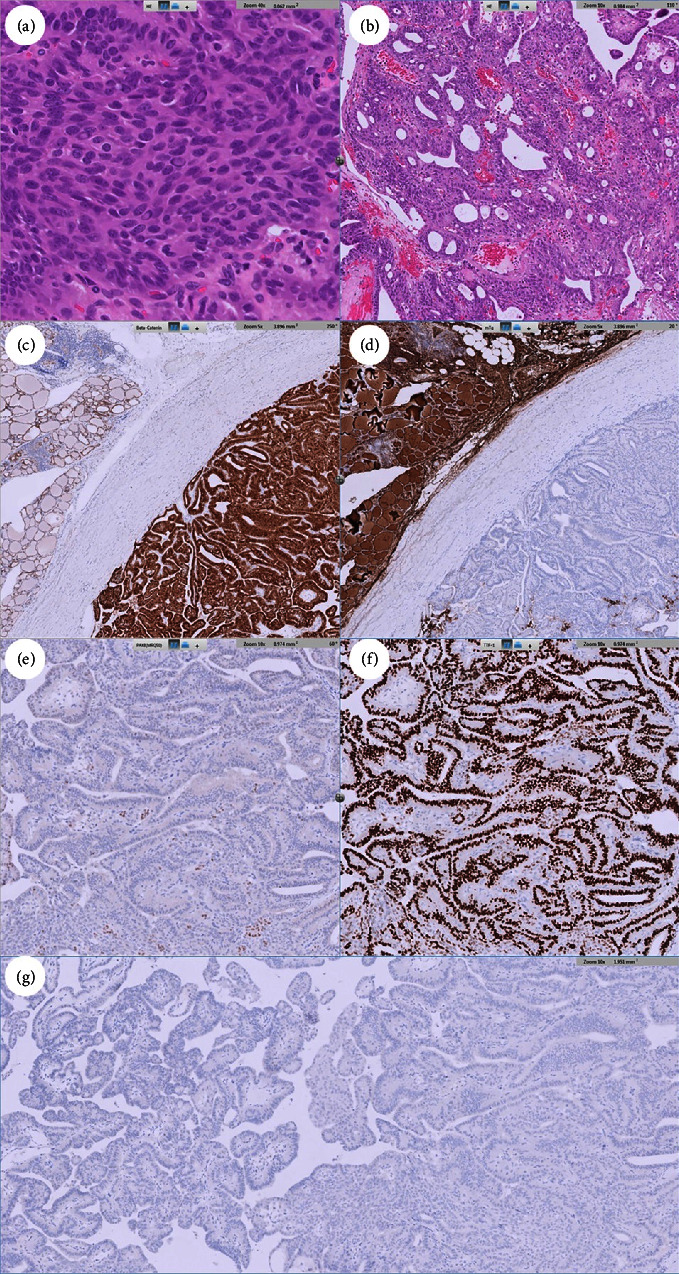
Results: A 31-year-old woman was found to have a thyroid nodule at the left lobe measuring 11.8 × 10.2 × 12.4 mm. Ultrasonography indicated a hypoechoic, solid nodule with regular margins. Cytology revealed a papillary structure of tall cells, leading to a PTC diagnosis. Nevertheless, the genetic analysis failed to detect mutations such as BRAF V600E, NRAS Q61R, NRAS Q61K, HRAS Q61R, or HRAS Q61K mutation or the fusion of CCDC6-RET, NCOA4-RET, PAX8-PPARG, ETV6-NTRK3, TPM3-NTRK1, IRF2BP2-NTRK1, or SQSTM1-NTRK1 in the aspirated follicular cells. The patient subsequently underwent total thyroidectomy with central lymph node dissection. Pathological examination revealed a cribriform pattern of spindle-shaped cells with morular areas. Immunohistochemical staining showed positive results for β-catenin and TTF-1, except in the morular regions, and negative results for PAX8, thyroglobulin, and BRAF (clone VE1). The diagnosis was confirmed to be cribriform morular thyroid carcinoma.
Conclusion: Significant cytological similarity exists between PTC and cribriform morular thyroid carcinoma. Preoperative genetic analysis is important to differentiate these two diseases. Cribriform morular thyroid carcinoma can be differentiated from common follicular-cell-derived tumors by the absence of typical mutations; the presence of nuclear and cytoplasmic expressions of β-catenin; the presence of TTF-1, except in morular areas; and the absence of thyroglobulin.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
