Murat Kara, Eren Erdogdu, Salih Duman, Gulnar Fatalizade, Berker Ozkan, Alper Toker
{"title":"对未经确诊但高度可疑的 I 期肺癌患者进行前期手术治疗的潜在生存益处。","authors":"Murat Kara, Eren Erdogdu, Salih Duman, Gulnar Fatalizade, Berker Ozkan, Alper Toker","doi":"10.5090/jcs.23.166","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with early-stage lung tumors that are highly suspicious for malignancy typically undergo a preoperative diagnostic workup, primarily through bronchoscopy or transthoracic biopsy. Those without a preoperative diagnosis may alternatively be treated with upfront surgery, contingent upon the potential for intraoperative diagnosis. Previous studies have yielded conflicting results regarding the impact of upfront surgery on the survival of these patients. Our study aimed to elucidate the effect of upfront surgery on the survival outcomes of patients undergoing surgery for early-stage lung cancer without a preoperative diagnosis.</p><p><strong>Methods: </strong>We analyzed the survival rate of 158 consecutive patients who underwent pulmonary resection for stage I lung cancer, either with or without a preoperative diagnosis.</p><p><strong>Results: </strong>A total of 86 patients (54%) underwent upfront surgery. This approach positively impacted both disease-free survival (p=0.031) and overall survival (p=0.017). However, no significant differences were observed across subgroups based on sex, smoking status, forced expiratory volume in 1 second, histologic tumor size, or histologic subtype. Univariate analysis identified upfront surgery (p=0.020), age (p=0.002), maximum standardized uptake value (SUVmax) exceeding 7 (p=0.001), and histological tumor size greater than 20 mm (p=0.009) as independent predictors. However, multivariate analysis indicated that only SUVmax greater than 7 (p=0.011) was a significant predictor of unfavorable survival.</p><p><strong>Conclusion: </strong>Upfront surgery does not appear to confer a survival advantage in patients with stage I lung cancer undergoing surgical intervention.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":" ","pages":"440-446"},"PeriodicalIF":1.0000,"publicationDate":"2024-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392711/pdf/","citationCount":"0","resultStr":"{\"title\":\"Potential Survival Benefit of Upfront Surgery for Lung Tumors Unconfirmed but Highly Suspicious for Stage I Lung Cancer.\",\"authors\":\"Murat Kara, Eren Erdogdu, Salih Duman, Gulnar Fatalizade, Berker Ozkan, Alper Toker\",\"doi\":\"10.5090/jcs.23.166\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with early-stage lung tumors that are highly suspicious for malignancy typically undergo a preoperative diagnostic workup, primarily through bronchoscopy or transthoracic biopsy. Those without a preoperative diagnosis may alternatively be treated with upfront surgery, contingent upon the potential for intraoperative diagnosis. Previous studies have yielded conflicting results regarding the impact of upfront surgery on the survival of these patients. Our study aimed to elucidate the effect of upfront surgery on the survival outcomes of patients undergoing surgery for early-stage lung cancer without a preoperative diagnosis.</p><p><strong>Methods: </strong>We analyzed the survival rate of 158 consecutive patients who underwent pulmonary resection for stage I lung cancer, either with or without a preoperative diagnosis.</p><p><strong>Results: </strong>A total of 86 patients (54%) underwent upfront surgery. This approach positively impacted both disease-free survival (p=0.031) and overall survival (p=0.017). However, no significant differences were observed across subgroups based on sex, smoking status, forced expiratory volume in 1 second, histologic tumor size, or histologic subtype. Univariate analysis identified upfront surgery (p=0.020), age (p=0.002), maximum standardized uptake value (SUVmax) exceeding 7 (p=0.001), and histological tumor size greater than 20 mm (p=0.009) as independent predictors. However, multivariate analysis indicated that only SUVmax greater than 7 (p=0.011) was a significant predictor of unfavorable survival.</p><p><strong>Conclusion: </strong>Upfront surgery does not appear to confer a survival advantage in patients with stage I lung cancer undergoing surgical intervention.</p>\",\"PeriodicalId\":34499,\"journal\":{\"name\":\"Journal of Chest Surgery\",\"volume\":\" \",\"pages\":\"440-446\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392711/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Chest Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5090/jcs.23.166\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.23.166","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/5 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:高度怀疑为恶性的早期肺部肿瘤患者通常要接受术前诊断,主要是通过支气管镜检查或经胸活检。没有术前诊断的患者可根据术中诊断的可能性,选择先期手术治疗。关于前期手术对这些患者生存期的影响,以往的研究得出了相互矛盾的结果。我们的研究旨在阐明前期手术对未经术前诊断的早期肺癌手术患者生存结果的影响:我们分析了连续 158 例接受肺切除术的 I 期肺癌患者的生存率,无论患者是否接受过术前诊断:共有 86 名患者(54%)接受了前期手术。这种方法对无病生存期(p=0.031)和总生存期(p=0.017)都有积极影响。然而,在基于性别、吸烟状况、1 秒用力呼气量、组织学肿瘤大小或组织学亚型的亚组中没有观察到明显差异。单变量分析发现,前期手术(p=0.020)、年龄(p=0.002)、最大标准化摄取值(SUVmax)超过 7(p=0.001)和组织学肿瘤大小超过 20 毫米(p=0.009)是独立的预测因素。然而,多变量分析表明,只有SUVmax大于7(p=0.011)才是不利生存的重要预测因素:结论:对于接受手术治疗的 I 期肺癌患者来说,前期手术似乎并不会带来生存优势。
Potential Survival Benefit of Upfront Surgery for Lung Tumors Unconfirmed but Highly Suspicious for Stage I Lung Cancer.
Background: Patients with early-stage lung tumors that are highly suspicious for malignancy typically undergo a preoperative diagnostic workup, primarily through bronchoscopy or transthoracic biopsy. Those without a preoperative diagnosis may alternatively be treated with upfront surgery, contingent upon the potential for intraoperative diagnosis. Previous studies have yielded conflicting results regarding the impact of upfront surgery on the survival of these patients. Our study aimed to elucidate the effect of upfront surgery on the survival outcomes of patients undergoing surgery for early-stage lung cancer without a preoperative diagnosis.
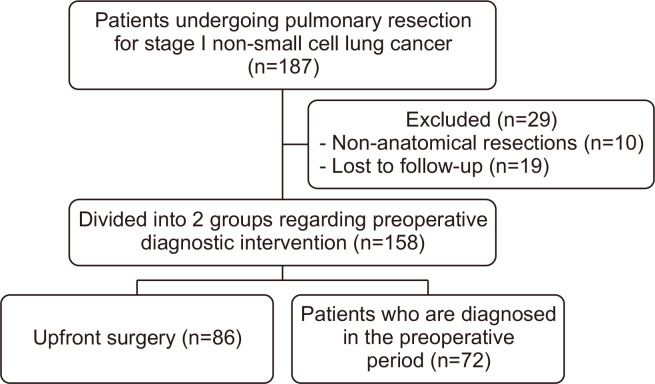
Methods: We analyzed the survival rate of 158 consecutive patients who underwent pulmonary resection for stage I lung cancer, either with or without a preoperative diagnosis.
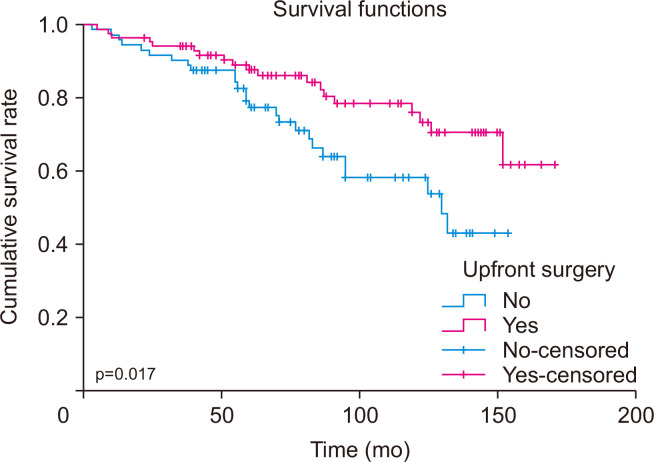
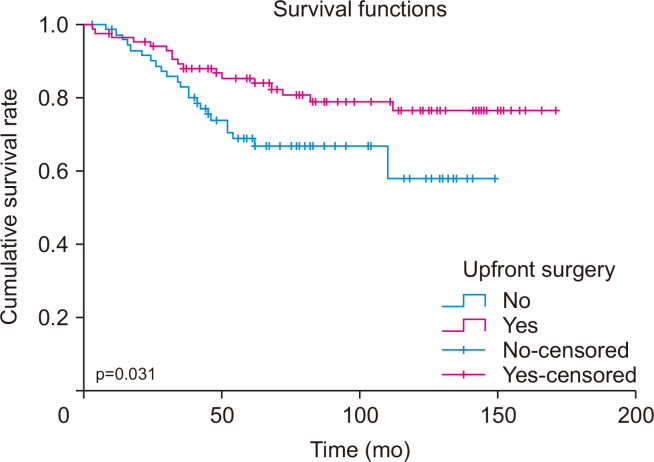
Results: A total of 86 patients (54%) underwent upfront surgery. This approach positively impacted both disease-free survival (p=0.031) and overall survival (p=0.017). However, no significant differences were observed across subgroups based on sex, smoking status, forced expiratory volume in 1 second, histologic tumor size, or histologic subtype. Univariate analysis identified upfront surgery (p=0.020), age (p=0.002), maximum standardized uptake value (SUVmax) exceeding 7 (p=0.001), and histological tumor size greater than 20 mm (p=0.009) as independent predictors. However, multivariate analysis indicated that only SUVmax greater than 7 (p=0.011) was a significant predictor of unfavorable survival.
Conclusion: Upfront surgery does not appear to confer a survival advantage in patients with stage I lung cancer undergoing surgical intervention.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
