{"title":"使用较低钙透析液浓度进行单次血液透析和血液滤过治疗期间成人的钙质量平衡","authors":"Roohi Chhabra, Andrew Davenport","doi":"10.1111/aor.14802","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Debate continues as to the optimum hemodialysis (HD) dialysate calcium concentration. Although current guidelines advocate 1.25–1.5 mmol/L, some investigators have suggested these may cause calcium gains. As such we investigated whether using dialysate calcium of 1.25 mmol/L risked calcium gains, and whether there were differences between hemodiafiltration and high flux HD.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We continuously collect an aliquot of effluent dialysate during dialysis sessions, and calculated dialysis calcium mass balance by the difference between the amount of calcium delivered as fresh dialysate and that lost in effluent dialysate.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We studied 106 stable outpatients, 64% male, mean age 64.4 ± 16.2 years, median dialysis vintage 32 (22–60) months. Most sessions (69%) used a 1.0 mmol/L calcium dialysate, with a median sessional loss of 13.7 (11.5–17.1) mmol, whereas using 1.25 mmol/L the median loss was 7.4 (4.9–10.1) mmol, but with 6.9% had a positive balance (<i>p</i> = 0.031 vs dialysate calcium 1.0 mmol/L). Most patients (85.8%) were treated by hemodiafiltration, but there was no difference in sessional losses (11.7 (8.4–15.8) vs 13.5 (8.1–16.8)) with high flux HD. Dialysis sessional calcium balance was associated with the use of lower dialysate calcium concentration (<i>β</i> −19.5, 95% confidence limits (95%CL) −27.7 to −11.3, <i>p</i> < 0.001), and sessional duration (<i>β</i> 0.07 (95% CL) 0.03–012, <i>p</i> = 0.002).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Ideally, the choice of dialysate calcium should be individualized, but clinicians should be aware, that even when using a dialysate calcium of 1.25 mmol/L, some patients are at risk of a calcium gain during hemodiafiltration and high-flux hemodialysis.</p>\n </section>\n </div>","PeriodicalId":8450,"journal":{"name":"Artificial organs","volume":"48 8","pages":"812-820"},"PeriodicalIF":2.3000,"publicationDate":"2024-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aor.14802","citationCount":"0","resultStr":"{\"title\":\"Calcium mass balance in adults during single hemodialysis and hemodiafiltration treatments using lower calcium dialysate concentrations\",\"authors\":\"Roohi Chhabra, Andrew Davenport\",\"doi\":\"10.1111/aor.14802\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Debate continues as to the optimum hemodialysis (HD) dialysate calcium concentration. Although current guidelines advocate 1.25–1.5 mmol/L, some investigators have suggested these may cause calcium gains. As such we investigated whether using dialysate calcium of 1.25 mmol/L risked calcium gains, and whether there were differences between hemodiafiltration and high flux HD.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We continuously collect an aliquot of effluent dialysate during dialysis sessions, and calculated dialysis calcium mass balance by the difference between the amount of calcium delivered as fresh dialysate and that lost in effluent dialysate.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We studied 106 stable outpatients, 64% male, mean age 64.4 ± 16.2 years, median dialysis vintage 32 (22–60) months. Most sessions (69%) used a 1.0 mmol/L calcium dialysate, with a median sessional loss of 13.7 (11.5–17.1) mmol, whereas using 1.25 mmol/L the median loss was 7.4 (4.9–10.1) mmol, but with 6.9% had a positive balance (<i>p</i> = 0.031 vs dialysate calcium 1.0 mmol/L). Most patients (85.8%) were treated by hemodiafiltration, but there was no difference in sessional losses (11.7 (8.4–15.8) vs 13.5 (8.1–16.8)) with high flux HD. Dialysis sessional calcium balance was associated with the use of lower dialysate calcium concentration (<i>β</i> −19.5, 95% confidence limits (95%CL) −27.7 to −11.3, <i>p</i> < 0.001), and sessional duration (<i>β</i> 0.07 (95% CL) 0.03–012, <i>p</i> = 0.002).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Ideally, the choice of dialysate calcium should be individualized, but clinicians should be aware, that even when using a dialysate calcium of 1.25 mmol/L, some patients are at risk of a calcium gain during hemodiafiltration and high-flux hemodialysis.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8450,\"journal\":{\"name\":\"Artificial organs\",\"volume\":\"48 8\",\"pages\":\"812-820\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-06-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aor.14802\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Artificial organs\",\"FirstCategoryId\":\"5\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/aor.14802\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENGINEERING, BIOMEDICAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Artificial organs","FirstCategoryId":"5","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/aor.14802","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
Calcium mass balance in adults during single hemodialysis and hemodiafiltration treatments using lower calcium dialysate concentrations
Background
Debate continues as to the optimum hemodialysis (HD) dialysate calcium concentration. Although current guidelines advocate 1.25–1.5 mmol/L, some investigators have suggested these may cause calcium gains. As such we investigated whether using dialysate calcium of 1.25 mmol/L risked calcium gains, and whether there were differences between hemodiafiltration and high flux HD.
Methods
We continuously collect an aliquot of effluent dialysate during dialysis sessions, and calculated dialysis calcium mass balance by the difference between the amount of calcium delivered as fresh dialysate and that lost in effluent dialysate.
Results
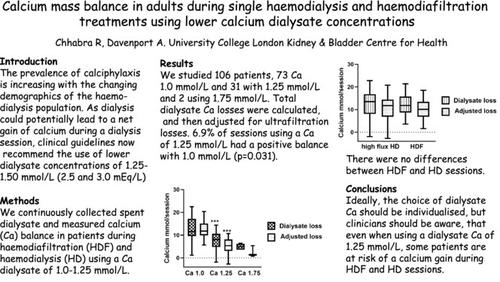
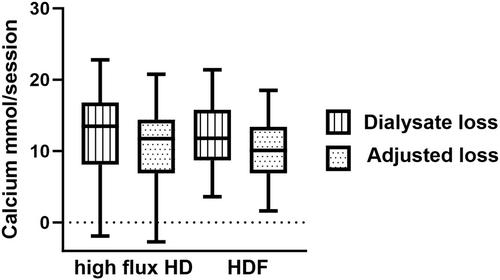
We studied 106 stable outpatients, 64% male, mean age 64.4 ± 16.2 years, median dialysis vintage 32 (22–60) months. Most sessions (69%) used a 1.0 mmol/L calcium dialysate, with a median sessional loss of 13.7 (11.5–17.1) mmol, whereas using 1.25 mmol/L the median loss was 7.4 (4.9–10.1) mmol, but with 6.9% had a positive balance (p = 0.031 vs dialysate calcium 1.0 mmol/L). Most patients (85.8%) were treated by hemodiafiltration, but there was no difference in sessional losses (11.7 (8.4–15.8) vs 13.5 (8.1–16.8)) with high flux HD. Dialysis sessional calcium balance was associated with the use of lower dialysate calcium concentration (β −19.5, 95% confidence limits (95%CL) −27.7 to −11.3, p < 0.001), and sessional duration (β 0.07 (95% CL) 0.03–012, p = 0.002).
Conclusion
Ideally, the choice of dialysate calcium should be individualized, but clinicians should be aware, that even when using a dialysate calcium of 1.25 mmol/L, some patients are at risk of a calcium gain during hemodiafiltration and high-flux hemodialysis.
期刊介绍:
Artificial Organs is the official peer reviewed journal of The International Federation for Artificial Organs (Members of the Federation are: The American Society for Artificial Internal Organs, The European Society for Artificial Organs, and The Japanese Society for Artificial Organs), The International Faculty for Artificial Organs, the International Society for Rotary Blood Pumps, The International Society for Pediatric Mechanical Cardiopulmonary Support, and the Vienna International Workshop on Functional Electrical Stimulation. Artificial Organs publishes original research articles dealing with developments in artificial organs applications and treatment modalities and their clinical applications worldwide. Membership in the Societies listed above is not a prerequisite for publication. Articles are published without charge to the author except for color figures and excess page charges as noted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
