Julianne M. Fallon Pharm.D., Emily McElhaney Pharm.D., Keith Anderson Pharm.D., Daniel A. Lewis Pharm.D., MBA, J. Bradley Williams Pharm.D.
{"title":"以药房为主导优化心力衰竭患者的护理转换","authors":"Julianne M. Fallon Pharm.D., Emily McElhaney Pharm.D., Keith Anderson Pharm.D., Daniel A. Lewis Pharm.D., MBA, J. Bradley Williams Pharm.D.","doi":"10.1002/jac5.1982","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Effective transitional care for patients with heart failure is essential to ensure optimal utilization of guideline-directed medical therapy. Clinical pharmacists and specially trained pharmacy technicians have unique skillsets that enable them to improve care transitions.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>To evaluate the implementation of a comprehensive pharmacy transitions of care program in an acute heart failure population.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A retrospective, single center, single-arm study evaluating pharmacy-delivered transitions of care services (admission and discharge medication reconciliation, medication cost assessment, medication counseling, bedside delivery of discharge medications, and post-discharge phone calls) for patients discharged from the heart failure service. The primary outcome was the completion rate of transitions of care services. Secondary outcomes included the medication intervention rate and types of interventions made, medication classes assessed for cost, discharge medication prescription captured, and 30-day all-cause readmissions.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Five hundred and ninety-five patients were eligible for the transitions of care program. Admission and discharge medication reconciliations were completed in 68.1% and 92.1% of patients, respectively. Medication cost assessments were completed for 39.8% of patients. Heart failure medication counseling prior to discharge was completed for 83.9% of patients. Discharge prescription capture rate was 56.5% and bedside prescription delivery was provided for 27.8% of patients. The discharge medication reconciliation intervention rate was 37.4%, with the most common intervention being dose adjustment. Post-discharge outreach was conducted for 229 patients, with education provided for 69.4% and an intervention rate of 43.7%. The 30-day all-cause readmission rate was lower for patients on the heart failure service compared with the institution (10.1% vs 16.5%).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>High rates of completion and utilization were identified after the implementation of a comprehensive pharmacy transitions of care program. Utilization of clinical pharmacists and pharmacy technicians during transitions of care improved medication access, patient education, and reduced medication-related problems.</p>\n </section>\n </div>","PeriodicalId":73966,"journal":{"name":"Journal of the American College of Clinical Pharmacy : JACCP","volume":"7 8","pages":"778-786"},"PeriodicalIF":1.5000,"publicationDate":"2024-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jac5.1982","citationCount":"0","resultStr":"{\"title\":\"Pharmacy-led optimization of transitions of care in patients with heart failure\",\"authors\":\"Julianne M. Fallon Pharm.D., Emily McElhaney Pharm.D., Keith Anderson Pharm.D., Daniel A. Lewis Pharm.D., MBA, J. Bradley Williams Pharm.D.\",\"doi\":\"10.1002/jac5.1982\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Effective transitional care for patients with heart failure is essential to ensure optimal utilization of guideline-directed medical therapy. Clinical pharmacists and specially trained pharmacy technicians have unique skillsets that enable them to improve care transitions.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>To evaluate the implementation of a comprehensive pharmacy transitions of care program in an acute heart failure population.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A retrospective, single center, single-arm study evaluating pharmacy-delivered transitions of care services (admission and discharge medication reconciliation, medication cost assessment, medication counseling, bedside delivery of discharge medications, and post-discharge phone calls) for patients discharged from the heart failure service. The primary outcome was the completion rate of transitions of care services. Secondary outcomes included the medication intervention rate and types of interventions made, medication classes assessed for cost, discharge medication prescription captured, and 30-day all-cause readmissions.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Five hundred and ninety-five patients were eligible for the transitions of care program. Admission and discharge medication reconciliations were completed in 68.1% and 92.1% of patients, respectively. Medication cost assessments were completed for 39.8% of patients. Heart failure medication counseling prior to discharge was completed for 83.9% of patients. Discharge prescription capture rate was 56.5% and bedside prescription delivery was provided for 27.8% of patients. The discharge medication reconciliation intervention rate was 37.4%, with the most common intervention being dose adjustment. Post-discharge outreach was conducted for 229 patients, with education provided for 69.4% and an intervention rate of 43.7%. The 30-day all-cause readmission rate was lower for patients on the heart failure service compared with the institution (10.1% vs 16.5%).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>High rates of completion and utilization were identified after the implementation of a comprehensive pharmacy transitions of care program. Utilization of clinical pharmacists and pharmacy technicians during transitions of care improved medication access, patient education, and reduced medication-related problems.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73966,\"journal\":{\"name\":\"Journal of the American College of Clinical Pharmacy : JACCP\",\"volume\":\"7 8\",\"pages\":\"778-786\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-06-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jac5.1982\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Clinical Pharmacy : JACCP\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://accpjournals.onlinelibrary.wiley.com/doi/10.1002/jac5.1982\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Clinical Pharmacy : JACCP","FirstCategoryId":"1085","ListUrlMain":"https://accpjournals.onlinelibrary.wiley.com/doi/10.1002/jac5.1982","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Pharmacy-led optimization of transitions of care in patients with heart failure
Introduction
Effective transitional care for patients with heart failure is essential to ensure optimal utilization of guideline-directed medical therapy. Clinical pharmacists and specially trained pharmacy technicians have unique skillsets that enable them to improve care transitions.
Objectives
To evaluate the implementation of a comprehensive pharmacy transitions of care program in an acute heart failure population.
Methods
A retrospective, single center, single-arm study evaluating pharmacy-delivered transitions of care services (admission and discharge medication reconciliation, medication cost assessment, medication counseling, bedside delivery of discharge medications, and post-discharge phone calls) for patients discharged from the heart failure service. The primary outcome was the completion rate of transitions of care services. Secondary outcomes included the medication intervention rate and types of interventions made, medication classes assessed for cost, discharge medication prescription captured, and 30-day all-cause readmissions.
Results
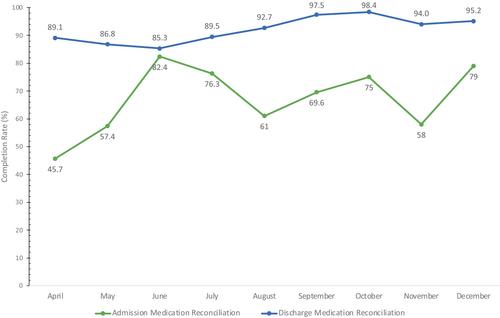
Five hundred and ninety-five patients were eligible for the transitions of care program. Admission and discharge medication reconciliations were completed in 68.1% and 92.1% of patients, respectively. Medication cost assessments were completed for 39.8% of patients. Heart failure medication counseling prior to discharge was completed for 83.9% of patients. Discharge prescription capture rate was 56.5% and bedside prescription delivery was provided for 27.8% of patients. The discharge medication reconciliation intervention rate was 37.4%, with the most common intervention being dose adjustment. Post-discharge outreach was conducted for 229 patients, with education provided for 69.4% and an intervention rate of 43.7%. The 30-day all-cause readmission rate was lower for patients on the heart failure service compared with the institution (10.1% vs 16.5%).
Conclusion
High rates of completion and utilization were identified after the implementation of a comprehensive pharmacy transitions of care program. Utilization of clinical pharmacists and pharmacy technicians during transitions of care improved medication access, patient education, and reduced medication-related problems.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
