{"title":"心血管手术后术前相位角与全因死亡率之间的关系:回顾性队列研究","authors":"Kenichi Shibata, Masataka Kameshima, Takuji Adachi, Hisako Kito, Chikako Tanaka, Taisei Sano, Mizuki Tanaka, Yoriyasu Suzuki, Mototsugu Tamaki, Hideki Kitamura","doi":"10.1002/jcsm.13514","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The importance of preoperative physical function assessment for post-operative intervention has been reported in older patients undergoing cardiovascular surgery. Phase angle (PhA), measured using bioelectrical impedance analysis, is an indicator of cellular health and integrity and is reported as a prognostic factor in several chronic diseases; however, its association with the long-term prognosis of cardiovascular surgery remains unclear. This study aimed to investigate the prognostic value of PhA for long-term mortality in patients undergoing cardiovascular surgery.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This retrospective cohort study included consecutive patients who underwent elective cardiovascular surgery between October 2016 and March 2021 at Nagoya Heart Center, Japan. PhA was assessed using bioelectrical impedance analysis before surgery, and physical function measures (gait speed, grip strength and short physical performance battery [SPPB]) were measured synchronously. The association between PhA and all-cause mortality after discharge was assessed using Kaplan–Meier and multivariate Cox regression analyses. The incremental prognostic value of PhA was compared with other physical function measures using net reclassification improvement (NRI) and integrated discrimination improvement (IDI).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 858 patients were included in the present analysis (mean age = 68.4 ± 11.9 years, 67.6% male). PhA positively correlated with body mass index (<i>ρ</i> = 0.38, <i>P</i> < 0.001), skeletal muscle mass index (<i>ρ</i> = 0.58, <i>P</i> < 0.001), usual gait speed (<i>ρ</i> = 0.44, <i>P</i> < 0.001), grip strength (<i>ρ</i> = 0.73, <i>P</i> < 0.001) and SPPB (<i>ρ</i> = 0.51, <i>P</i> < 0.001). The mean follow-up period, within which 44 (4.7%) died, was 908.9 ± 499.9 days for the entire cohort. Kaplan–Meier survival curves based on the PhA tertiles showed that higher PhA was associated with better survival (log-rank test, <i>P</i> < 0.001). The Cox regression analysis showed the independent association of PhA with mortality risk (hazard ratio: 0.91 per 0.1° increment; 95% confidence interval [CI]: 0.87–0.95; <i>P</i> < 0.001). The NRI and IDI showed significant improvements in predicting mortality after adding PhA to the clinical model consisting of age, sex and cardiac and renal function (NRI: 0.426, 95% CI: 0.124–0.729, <i>P</i> = 0.006; IDI: 0.037, 95% CI: 0.012–0.062, <i>P</i> = 0.003). The predictive model consisting of the clinical model and PhA was superior to the model consisting of the clinical model and each of the other physical function indicators (<i>P</i> < 0.05).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>PhA correlated with physical function and independently predicted long-term mortality after cardiovascular surgery. The additive prognostic value of PhA compared with the other physical function measures suggests the clinical usefulness of preoperative PhA for risk stratification in planning post-operative treatment and rehabilitation.</p>\n </section>\n </div>","PeriodicalId":48911,"journal":{"name":"Journal of Cachexia Sarcopenia and Muscle","volume":"15 4","pages":"1558-1567"},"PeriodicalIF":9.1000,"publicationDate":"2024-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11294016/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association between preoperative phase angle and all-cause mortality after cardiovascular surgery: A retrospective cohort study\",\"authors\":\"Kenichi Shibata, Masataka Kameshima, Takuji Adachi, Hisako Kito, Chikako Tanaka, Taisei Sano, Mizuki Tanaka, Yoriyasu Suzuki, Mototsugu Tamaki, Hideki Kitamura\",\"doi\":\"10.1002/jcsm.13514\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>The importance of preoperative physical function assessment for post-operative intervention has been reported in older patients undergoing cardiovascular surgery. Phase angle (PhA), measured using bioelectrical impedance analysis, is an indicator of cellular health and integrity and is reported as a prognostic factor in several chronic diseases; however, its association with the long-term prognosis of cardiovascular surgery remains unclear. This study aimed to investigate the prognostic value of PhA for long-term mortality in patients undergoing cardiovascular surgery.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This retrospective cohort study included consecutive patients who underwent elective cardiovascular surgery between October 2016 and March 2021 at Nagoya Heart Center, Japan. PhA was assessed using bioelectrical impedance analysis before surgery, and physical function measures (gait speed, grip strength and short physical performance battery [SPPB]) were measured synchronously. The association between PhA and all-cause mortality after discharge was assessed using Kaplan–Meier and multivariate Cox regression analyses. The incremental prognostic value of PhA was compared with other physical function measures using net reclassification improvement (NRI) and integrated discrimination improvement (IDI).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 858 patients were included in the present analysis (mean age = 68.4 ± 11.9 years, 67.6% male). PhA positively correlated with body mass index (<i>ρ</i> = 0.38, <i>P</i> < 0.001), skeletal muscle mass index (<i>ρ</i> = 0.58, <i>P</i> < 0.001), usual gait speed (<i>ρ</i> = 0.44, <i>P</i> < 0.001), grip strength (<i>ρ</i> = 0.73, <i>P</i> < 0.001) and SPPB (<i>ρ</i> = 0.51, <i>P</i> < 0.001). The mean follow-up period, within which 44 (4.7%) died, was 908.9 ± 499.9 days for the entire cohort. Kaplan–Meier survival curves based on the PhA tertiles showed that higher PhA was associated with better survival (log-rank test, <i>P</i> < 0.001). The Cox regression analysis showed the independent association of PhA with mortality risk (hazard ratio: 0.91 per 0.1° increment; 95% confidence interval [CI]: 0.87–0.95; <i>P</i> < 0.001). The NRI and IDI showed significant improvements in predicting mortality after adding PhA to the clinical model consisting of age, sex and cardiac and renal function (NRI: 0.426, 95% CI: 0.124–0.729, <i>P</i> = 0.006; IDI: 0.037, 95% CI: 0.012–0.062, <i>P</i> = 0.003). The predictive model consisting of the clinical model and PhA was superior to the model consisting of the clinical model and each of the other physical function indicators (<i>P</i> < 0.05).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>PhA correlated with physical function and independently predicted long-term mortality after cardiovascular surgery. The additive prognostic value of PhA compared with the other physical function measures suggests the clinical usefulness of preoperative PhA for risk stratification in planning post-operative treatment and rehabilitation.</p>\\n </section>\\n </div>\",\"PeriodicalId\":48911,\"journal\":{\"name\":\"Journal of Cachexia Sarcopenia and Muscle\",\"volume\":\"15 4\",\"pages\":\"1558-1567\"},\"PeriodicalIF\":9.1000,\"publicationDate\":\"2024-06-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11294016/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cachexia Sarcopenia and Muscle\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13514\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cachexia Sarcopenia and Muscle","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13514","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Association between preoperative phase angle and all-cause mortality after cardiovascular surgery: A retrospective cohort study
Background
The importance of preoperative physical function assessment for post-operative intervention has been reported in older patients undergoing cardiovascular surgery. Phase angle (PhA), measured using bioelectrical impedance analysis, is an indicator of cellular health and integrity and is reported as a prognostic factor in several chronic diseases; however, its association with the long-term prognosis of cardiovascular surgery remains unclear. This study aimed to investigate the prognostic value of PhA for long-term mortality in patients undergoing cardiovascular surgery.
Methods
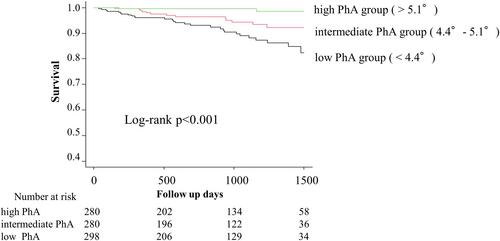
This retrospective cohort study included consecutive patients who underwent elective cardiovascular surgery between October 2016 and March 2021 at Nagoya Heart Center, Japan. PhA was assessed using bioelectrical impedance analysis before surgery, and physical function measures (gait speed, grip strength and short physical performance battery [SPPB]) were measured synchronously. The association between PhA and all-cause mortality after discharge was assessed using Kaplan–Meier and multivariate Cox regression analyses. The incremental prognostic value of PhA was compared with other physical function measures using net reclassification improvement (NRI) and integrated discrimination improvement (IDI).
Results
A total of 858 patients were included in the present analysis (mean age = 68.4 ± 11.9 years, 67.6% male). PhA positively correlated with body mass index (ρ = 0.38, P < 0.001), skeletal muscle mass index (ρ = 0.58, P < 0.001), usual gait speed (ρ = 0.44, P < 0.001), grip strength (ρ = 0.73, P < 0.001) and SPPB (ρ = 0.51, P < 0.001). The mean follow-up period, within which 44 (4.7%) died, was 908.9 ± 499.9 days for the entire cohort. Kaplan–Meier survival curves based on the PhA tertiles showed that higher PhA was associated with better survival (log-rank test, P < 0.001). The Cox regression analysis showed the independent association of PhA with mortality risk (hazard ratio: 0.91 per 0.1° increment; 95% confidence interval [CI]: 0.87–0.95; P < 0.001). The NRI and IDI showed significant improvements in predicting mortality after adding PhA to the clinical model consisting of age, sex and cardiac and renal function (NRI: 0.426, 95% CI: 0.124–0.729, P = 0.006; IDI: 0.037, 95% CI: 0.012–0.062, P = 0.003). The predictive model consisting of the clinical model and PhA was superior to the model consisting of the clinical model and each of the other physical function indicators (P < 0.05).
Conclusions
PhA correlated with physical function and independently predicted long-term mortality after cardiovascular surgery. The additive prognostic value of PhA compared with the other physical function measures suggests the clinical usefulness of preoperative PhA for risk stratification in planning post-operative treatment and rehabilitation.
期刊介绍:
The Journal of Cachexia, Sarcopenia and Muscle is a peer-reviewed international journal dedicated to publishing materials related to cachexia and sarcopenia, as well as body composition and its physiological and pathophysiological changes across the lifespan and in response to various illnesses from all fields of life sciences. The journal aims to provide a reliable resource for professionals interested in related research or involved in the clinical care of affected patients, such as those suffering from AIDS, cancer, chronic heart failure, chronic lung disease, liver cirrhosis, chronic kidney failure, rheumatoid arthritis, or sepsis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
