Alessandro Martinino, Kushan D L Nanayakkara, Brij Madhok, Geoffrey Yuet Mun Wong, Mohamed Abouelazayem, Juan Pablo Scarano Pereira, Ishaan Wazir, Vignesh Balasubaramaniam, Amira Said, Cláudia Marques, Amr Abdelbaeth, Khayry Al-Shami, Muna Albashari, Akram Alkaseek, Mohammad Abdullah Almayouf, Mohammad Aloulou, Awadh Robaan Alqahtan, Alan Askari, Meena Faiez Assad Attia, Ahmed K Awad, Muhammed Rasid Aykota, Nicolae Bacalbasa, Francisco J Barrera-Rodriguez, Domenico Benavoli, Srikar Billa, Vincenzo Borrelli, İsmail Çalıkoğlu, Michela Campanelli, Miguel A Carbajo, Sharfuddin Chowdhury, Luca Cristin, Giovanni Dapri, Zhiyong Dong, Mohamad Hayssam Elfawal, Amr Elgazar, Muhammed Elhadi, Paolo Gentileschi, Yitka Graham, Bassel Haj, Joseph Andrew Johnson, Abd-Elfattah Morsi Kalmoush, Ayman Kamal, Anna Kamocka, Almu'atasim Khamees, Giorgio Lisi, Edgard Efren Lozada Hernandez, Giuseppe M Marinari, Gennaro Martines, Serhat Meric, Fernando Mier, Ahmed Mohamed Ali, Diyaaldeen Mohammed, Karim Mostafa Mohamed, Francesk Mulita, Mario Musella, William Edward O'Malley, Stefano Olmi, Taryel Omarov, Omnya Osama, HMinali R Perera, Giovanni Piscitelli, Tigran Poghosyan, David Ramírez, Masoud Rezvani, Rui Ribeiro, Aaron Sabbota, Nasser Sakran, Khaled Ahmad Sawaftah, Kaci Schiavone, Ozan Şen, Maria Sotiropoulou, Nicola Tartaglia, Merve Tokocin, Manuela Trotta, Ahmet Gökhan Türkçapar, Matteo Uccelli, Cesar Vargas, Georgios -Ioannis Verras, Cunchuan Wang, Zhuoqi Wei, Wah Yang, Carlos Zerrweck, Eloise Owen, Georgios V Gkoutos, Victor Roth Cardoso, Rishi Singhal, Kamal Mahawar
{"title":"原发性减肥手术联合其他手术的全球 30 天发病率和死亡率:BLEND 研究。","authors":"Alessandro Martinino, Kushan D L Nanayakkara, Brij Madhok, Geoffrey Yuet Mun Wong, Mohamed Abouelazayem, Juan Pablo Scarano Pereira, Ishaan Wazir, Vignesh Balasubaramaniam, Amira Said, Cláudia Marques, Amr Abdelbaeth, Khayry Al-Shami, Muna Albashari, Akram Alkaseek, Mohammad Abdullah Almayouf, Mohammad Aloulou, Awadh Robaan Alqahtan, Alan Askari, Meena Faiez Assad Attia, Ahmed K Awad, Muhammed Rasid Aykota, Nicolae Bacalbasa, Francisco J Barrera-Rodriguez, Domenico Benavoli, Srikar Billa, Vincenzo Borrelli, İsmail Çalıkoğlu, Michela Campanelli, Miguel A Carbajo, Sharfuddin Chowdhury, Luca Cristin, Giovanni Dapri, Zhiyong Dong, Mohamad Hayssam Elfawal, Amr Elgazar, Muhammed Elhadi, Paolo Gentileschi, Yitka Graham, Bassel Haj, Joseph Andrew Johnson, Abd-Elfattah Morsi Kalmoush, Ayman Kamal, Anna Kamocka, Almu'atasim Khamees, Giorgio Lisi, Edgard Efren Lozada Hernandez, Giuseppe M Marinari, Gennaro Martines, Serhat Meric, Fernando Mier, Ahmed Mohamed Ali, Diyaaldeen Mohammed, Karim Mostafa Mohamed, Francesk Mulita, Mario Musella, William Edward O'Malley, Stefano Olmi, Taryel Omarov, Omnya Osama, HMinali R Perera, Giovanni Piscitelli, Tigran Poghosyan, David Ramírez, Masoud Rezvani, Rui Ribeiro, Aaron Sabbota, Nasser Sakran, Khaled Ahmad Sawaftah, Kaci Schiavone, Ozan Şen, Maria Sotiropoulou, Nicola Tartaglia, Merve Tokocin, Manuela Trotta, Ahmet Gökhan Türkçapar, Matteo Uccelli, Cesar Vargas, Georgios -Ioannis Verras, Cunchuan Wang, Zhuoqi Wei, Wah Yang, Carlos Zerrweck, Eloise Owen, Georgios V Gkoutos, Victor Roth Cardoso, Rishi Singhal, Kamal Mahawar","doi":"10.1007/s11695-024-07296-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>No robust data are available on the safety of primary bariatric and metabolic surgery (BMS) alone compared to primary BMS combined with other procedures.</p><p><strong>Objectives: </strong>The objective of this study is to collect a 30-day mortality and morbidity of primary BMS combined with cholecystectomy, ventral hernia repair, or hiatal hernia repair.</p><p><strong>Setting: </strong>This is as an international, multicenter, prospective, and observational audit of patients undergoing primary BMS combined with one or more additional procedures.</p><p><strong>Methods: </strong>The audit took place from January 1 to June 30, 2022. A descriptive analysis was conducted. A propensity score matching analysis compared the BLEND study patients with those from the GENEVA cohort to obtain objective evaluation between combined procedures and primary BMS alone.</p><p><strong>Results: </strong>A total of 75 centers submitted data on 1036 patients. Sleeve gastrectomy was the most commonly primary BMS (N = 653, 63%), and hiatal hernia repair was the most commonly concomitant procedure (N = 447, 43.1%). RYGB accounted for the highest percentage (20.6%) of a 30-day morbidity, followed by SG (10.5%). More than one combined procedures had the highest morbidities among all combinations (17.1%). Out of overall 134 complications, 129 (96.2%) were Clavien-Dindo I-III, and 4 were CD V. Patients who underwent a primary bariatric surgery combined with another procedure had a pronounced increase in a 30-day complication rate compared with patients who underwent only BMS (12.7% vs. 7.1%).</p><p><strong>Conclusion: </strong>Combining BMS with another procedure increases the risk of complications, but most are minor and require no further treatment. Combined procedures with primary BMS is a viable option to consider in selected patients following multi-disciplinary discussion.</p>","PeriodicalId":19460,"journal":{"name":"Obesity Surgery","volume":" ","pages":"4152-4165"},"PeriodicalIF":3.1000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Global 30-Day Morbidity and Mortality of Primary Bariatric Surgery Combined with Another Procedure: The BLEND Study.\",\"authors\":\"Alessandro Martinino, Kushan D L Nanayakkara, Brij Madhok, Geoffrey Yuet Mun Wong, Mohamed Abouelazayem, Juan Pablo Scarano Pereira, Ishaan Wazir, Vignesh Balasubaramaniam, Amira Said, Cláudia Marques, Amr Abdelbaeth, Khayry Al-Shami, Muna Albashari, Akram Alkaseek, Mohammad Abdullah Almayouf, Mohammad Aloulou, Awadh Robaan Alqahtan, Alan Askari, Meena Faiez Assad Attia, Ahmed K Awad, Muhammed Rasid Aykota, Nicolae Bacalbasa, Francisco J Barrera-Rodriguez, Domenico Benavoli, Srikar Billa, Vincenzo Borrelli, İsmail Çalıkoğlu, Michela Campanelli, Miguel A Carbajo, Sharfuddin Chowdhury, Luca Cristin, Giovanni Dapri, Zhiyong Dong, Mohamad Hayssam Elfawal, Amr Elgazar, Muhammed Elhadi, Paolo Gentileschi, Yitka Graham, Bassel Haj, Joseph Andrew Johnson, Abd-Elfattah Morsi Kalmoush, Ayman Kamal, Anna Kamocka, Almu'atasim Khamees, Giorgio Lisi, Edgard Efren Lozada Hernandez, Giuseppe M Marinari, Gennaro Martines, Serhat Meric, Fernando Mier, Ahmed Mohamed Ali, Diyaaldeen Mohammed, Karim Mostafa Mohamed, Francesk Mulita, Mario Musella, William Edward O'Malley, Stefano Olmi, Taryel Omarov, Omnya Osama, HMinali R Perera, Giovanni Piscitelli, Tigran Poghosyan, David Ramírez, Masoud Rezvani, Rui Ribeiro, Aaron Sabbota, Nasser Sakran, Khaled Ahmad Sawaftah, Kaci Schiavone, Ozan Şen, Maria Sotiropoulou, Nicola Tartaglia, Merve Tokocin, Manuela Trotta, Ahmet Gökhan Türkçapar, Matteo Uccelli, Cesar Vargas, Georgios -Ioannis Verras, Cunchuan Wang, Zhuoqi Wei, Wah Yang, Carlos Zerrweck, Eloise Owen, Georgios V Gkoutos, Victor Roth Cardoso, Rishi Singhal, Kamal Mahawar\",\"doi\":\"10.1007/s11695-024-07296-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>No robust data are available on the safety of primary bariatric and metabolic surgery (BMS) alone compared to primary BMS combined with other procedures.</p><p><strong>Objectives: </strong>The objective of this study is to collect a 30-day mortality and morbidity of primary BMS combined with cholecystectomy, ventral hernia repair, or hiatal hernia repair.</p><p><strong>Setting: </strong>This is as an international, multicenter, prospective, and observational audit of patients undergoing primary BMS combined with one or more additional procedures.</p><p><strong>Methods: </strong>The audit took place from January 1 to June 30, 2022. A descriptive analysis was conducted. A propensity score matching analysis compared the BLEND study patients with those from the GENEVA cohort to obtain objective evaluation between combined procedures and primary BMS alone.</p><p><strong>Results: </strong>A total of 75 centers submitted data on 1036 patients. Sleeve gastrectomy was the most commonly primary BMS (N = 653, 63%), and hiatal hernia repair was the most commonly concomitant procedure (N = 447, 43.1%). RYGB accounted for the highest percentage (20.6%) of a 30-day morbidity, followed by SG (10.5%). More than one combined procedures had the highest morbidities among all combinations (17.1%). Out of overall 134 complications, 129 (96.2%) were Clavien-Dindo I-III, and 4 were CD V. Patients who underwent a primary bariatric surgery combined with another procedure had a pronounced increase in a 30-day complication rate compared with patients who underwent only BMS (12.7% vs. 7.1%).</p><p><strong>Conclusion: </strong>Combining BMS with another procedure increases the risk of complications, but most are minor and require no further treatment. Combined procedures with primary BMS is a viable option to consider in selected patients following multi-disciplinary discussion.</p>\",\"PeriodicalId\":19460,\"journal\":{\"name\":\"Obesity Surgery\",\"volume\":\" \",\"pages\":\"4152-4165\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Obesity Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11695-024-07296-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11695-024-07296-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/13 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
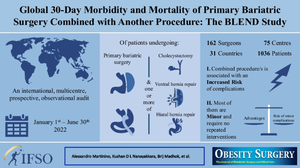
Global 30-Day Morbidity and Mortality of Primary Bariatric Surgery Combined with Another Procedure: The BLEND Study.
Background: No robust data are available on the safety of primary bariatric and metabolic surgery (BMS) alone compared to primary BMS combined with other procedures.
Objectives: The objective of this study is to collect a 30-day mortality and morbidity of primary BMS combined with cholecystectomy, ventral hernia repair, or hiatal hernia repair.
Setting: This is as an international, multicenter, prospective, and observational audit of patients undergoing primary BMS combined with one or more additional procedures.
Methods: The audit took place from January 1 to June 30, 2022. A descriptive analysis was conducted. A propensity score matching analysis compared the BLEND study patients with those from the GENEVA cohort to obtain objective evaluation between combined procedures and primary BMS alone.
Results: A total of 75 centers submitted data on 1036 patients. Sleeve gastrectomy was the most commonly primary BMS (N = 653, 63%), and hiatal hernia repair was the most commonly concomitant procedure (N = 447, 43.1%). RYGB accounted for the highest percentage (20.6%) of a 30-day morbidity, followed by SG (10.5%). More than one combined procedures had the highest morbidities among all combinations (17.1%). Out of overall 134 complications, 129 (96.2%) were Clavien-Dindo I-III, and 4 were CD V. Patients who underwent a primary bariatric surgery combined with another procedure had a pronounced increase in a 30-day complication rate compared with patients who underwent only BMS (12.7% vs. 7.1%).
Conclusion: Combining BMS with another procedure increases the risk of complications, but most are minor and require no further treatment. Combined procedures with primary BMS is a viable option to consider in selected patients following multi-disciplinary discussion.
期刊介绍:
Obesity Surgery is the official journal of the International Federation for the Surgery of Obesity and metabolic disorders (IFSO). A journal for bariatric/metabolic surgeons, Obesity Surgery provides an international, interdisciplinary forum for communicating the latest research, surgical and laparoscopic techniques, for treatment of massive obesity and metabolic disorders. Topics covered include original research, clinical reports, current status, guidelines, historical notes, invited commentaries, letters to the editor, medicolegal issues, meeting abstracts, modern surgery/technical innovations, new concepts, reviews, scholarly presentations and opinions.
Obesity Surgery benefits surgeons performing obesity/metabolic surgery, general surgeons and surgical residents, endoscopists, anesthetists, support staff, nurses, dietitians, psychiatrists, psychologists, plastic surgeons, internists including endocrinologists and diabetologists, nutritional scientists, and those dealing with eating disorders.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
