Kareem A Wahid, Onur Sahin, Suprateek Kundu, Diana Lin, Anthony Alanis, Salik Tehami, Serageldin Kamel, Simon Duke, Michael V Sherer, Mathis Rasmussen, Stine Korreman, David Fuentes, Michael Cislo, Benjamin E Nelms, John P Christodouleas, James D Murphy, Abdallah S R Mohamed, Renjie He, Mohammed A Naser, Erin F Gillespie, Clifton D Fuller
{"title":"放射肿瘤学家人口统计因素与分段相似性基准之间的关联:利用贝叶斯估计从众包挑战中获得的启示。","authors":"Kareem A Wahid, Onur Sahin, Suprateek Kundu, Diana Lin, Anthony Alanis, Salik Tehami, Serageldin Kamel, Simon Duke, Michael V Sherer, Mathis Rasmussen, Stine Korreman, David Fuentes, Michael Cislo, Benjamin E Nelms, John P Christodouleas, James D Murphy, Abdallah S R Mohamed, Renjie He, Mohammed A Naser, Erin F Gillespie, Clifton D Fuller","doi":"10.1200/CCI.23.00174","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The quality of radiotherapy auto-segmentation training data, primarily derived from clinician observers, is of utmost importance. However, the factors influencing the quality of clinician-derived segmentations are poorly understood; our study aims to quantify these factors.</p><p><strong>Methods: </strong>Organ at risk (OAR) and tumor-related segmentations provided by radiation oncologists from the Contouring Collaborative for Consensus in Radiation Oncology data set were used. Segmentations were derived from five disease sites: breast, sarcoma, head and neck (H&N), gynecologic (GYN), and GI. Segmentation quality was determined on a structure-by-structure basis by comparing the observer segmentations with an expert-derived consensus, which served as a reference standard benchmark. The Dice similarity coefficient (DSC) was primarily used as a metric for the comparisons. DSC was stratified into binary groups on the basis of structure-specific expert-derived interobserver variability (IOV) cutoffs. Generalized linear mixed-effects models using Bayesian estimation were used to investigate the association between demographic variables and the binarized DSC for each disease site. Variables with a highest density interval excluding zero were considered to substantially affect the outcome measure.</p><p><strong>Results: </strong>Five hundred seventy-four, 110, 452, 112, and 48 segmentations were used for the breast, sarcoma, H&N, GYN, and GI cases, respectively. The median percentage of segmentations that crossed the expert DSC IOV cutoff when stratified by structure type was 55% and 31% for OARs and tumors, respectively. Regression analysis revealed that the structure being tumor-related had a substantial negative impact on binarized DSC for the breast, sarcoma, H&N, and GI cases. There were no recurring relationships between segmentation quality and demographic variables across the cases, with most variables demonstrating large standard deviations.</p><p><strong>Conclusion: </strong>Our study highlights substantial uncertainty surrounding conventionally presumed factors influencing segmentation quality relative to benchmarks.</p>","PeriodicalId":51626,"journal":{"name":"JCO Clinical Cancer Informatics","volume":"8 ","pages":"e2300174"},"PeriodicalIF":3.6000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11214868/pdf/","citationCount":"0","resultStr":"{\"title\":\"Associations Between Radiation Oncologist Demographic Factors and Segmentation Similarity Benchmarks: Insights From a Crowd-Sourced Challenge Using Bayesian Estimation.\",\"authors\":\"Kareem A Wahid, Onur Sahin, Suprateek Kundu, Diana Lin, Anthony Alanis, Salik Tehami, Serageldin Kamel, Simon Duke, Michael V Sherer, Mathis Rasmussen, Stine Korreman, David Fuentes, Michael Cislo, Benjamin E Nelms, John P Christodouleas, James D Murphy, Abdallah S R Mohamed, Renjie He, Mohammed A Naser, Erin F Gillespie, Clifton D Fuller\",\"doi\":\"10.1200/CCI.23.00174\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The quality of radiotherapy auto-segmentation training data, primarily derived from clinician observers, is of utmost importance. However, the factors influencing the quality of clinician-derived segmentations are poorly understood; our study aims to quantify these factors.</p><p><strong>Methods: </strong>Organ at risk (OAR) and tumor-related segmentations provided by radiation oncologists from the Contouring Collaborative for Consensus in Radiation Oncology data set were used. Segmentations were derived from five disease sites: breast, sarcoma, head and neck (H&N), gynecologic (GYN), and GI. Segmentation quality was determined on a structure-by-structure basis by comparing the observer segmentations with an expert-derived consensus, which served as a reference standard benchmark. The Dice similarity coefficient (DSC) was primarily used as a metric for the comparisons. DSC was stratified into binary groups on the basis of structure-specific expert-derived interobserver variability (IOV) cutoffs. Generalized linear mixed-effects models using Bayesian estimation were used to investigate the association between demographic variables and the binarized DSC for each disease site. Variables with a highest density interval excluding zero were considered to substantially affect the outcome measure.</p><p><strong>Results: </strong>Five hundred seventy-four, 110, 452, 112, and 48 segmentations were used for the breast, sarcoma, H&N, GYN, and GI cases, respectively. The median percentage of segmentations that crossed the expert DSC IOV cutoff when stratified by structure type was 55% and 31% for OARs and tumors, respectively. Regression analysis revealed that the structure being tumor-related had a substantial negative impact on binarized DSC for the breast, sarcoma, H&N, and GI cases. There were no recurring relationships between segmentation quality and demographic variables across the cases, with most variables demonstrating large standard deviations.</p><p><strong>Conclusion: </strong>Our study highlights substantial uncertainty surrounding conventionally presumed factors influencing segmentation quality relative to benchmarks.</p>\",\"PeriodicalId\":51626,\"journal\":{\"name\":\"JCO Clinical Cancer Informatics\",\"volume\":\"8 \",\"pages\":\"e2300174\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11214868/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCO Clinical Cancer Informatics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1200/CCI.23.00174\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCO Clinical Cancer Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1200/CCI.23.00174","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Associations Between Radiation Oncologist Demographic Factors and Segmentation Similarity Benchmarks: Insights From a Crowd-Sourced Challenge Using Bayesian Estimation.
Purpose: The quality of radiotherapy auto-segmentation training data, primarily derived from clinician observers, is of utmost importance. However, the factors influencing the quality of clinician-derived segmentations are poorly understood; our study aims to quantify these factors.
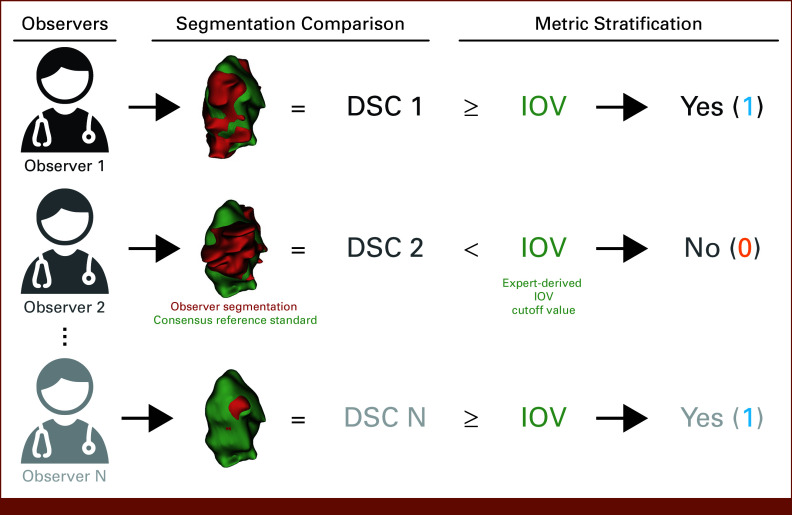
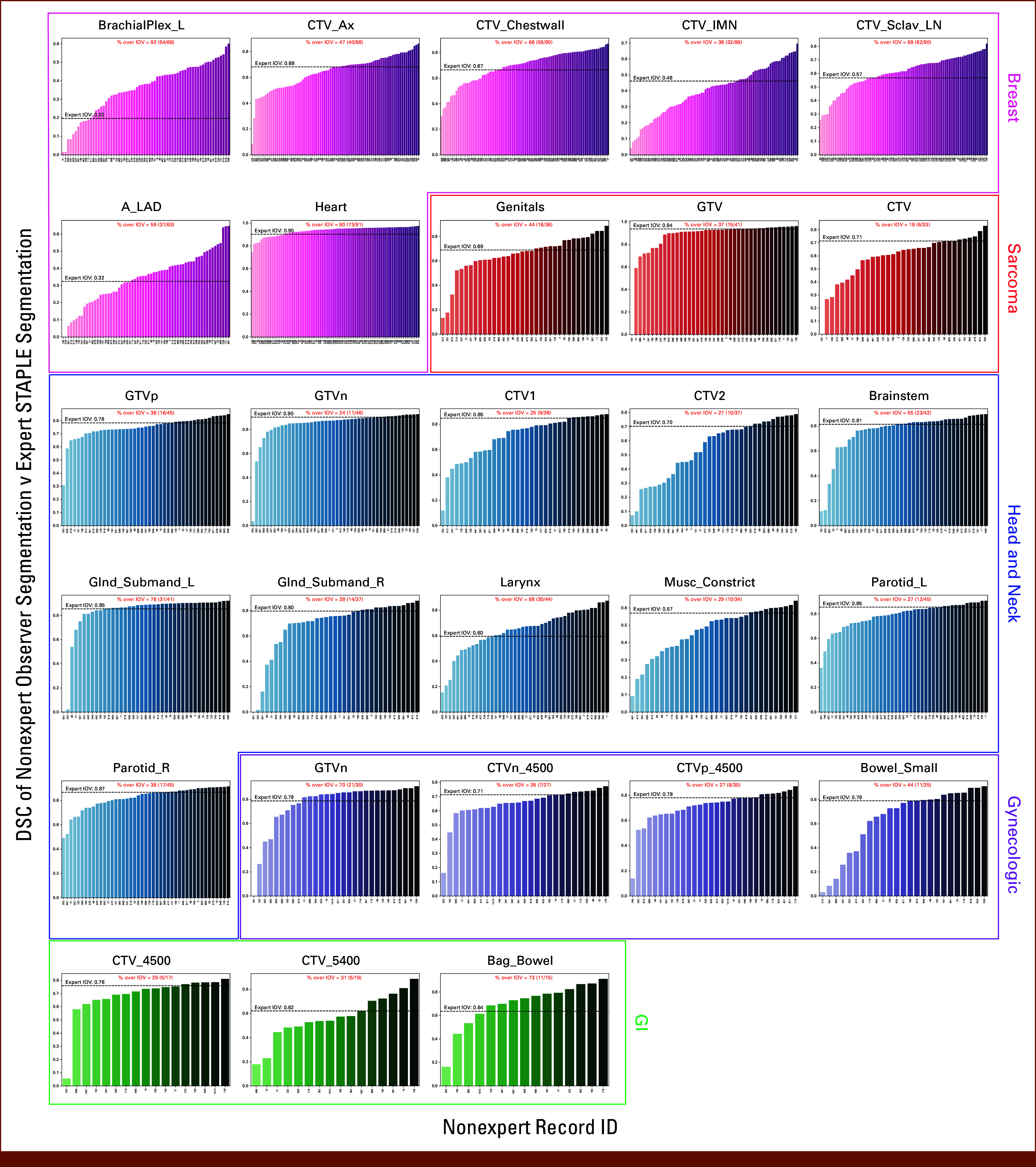
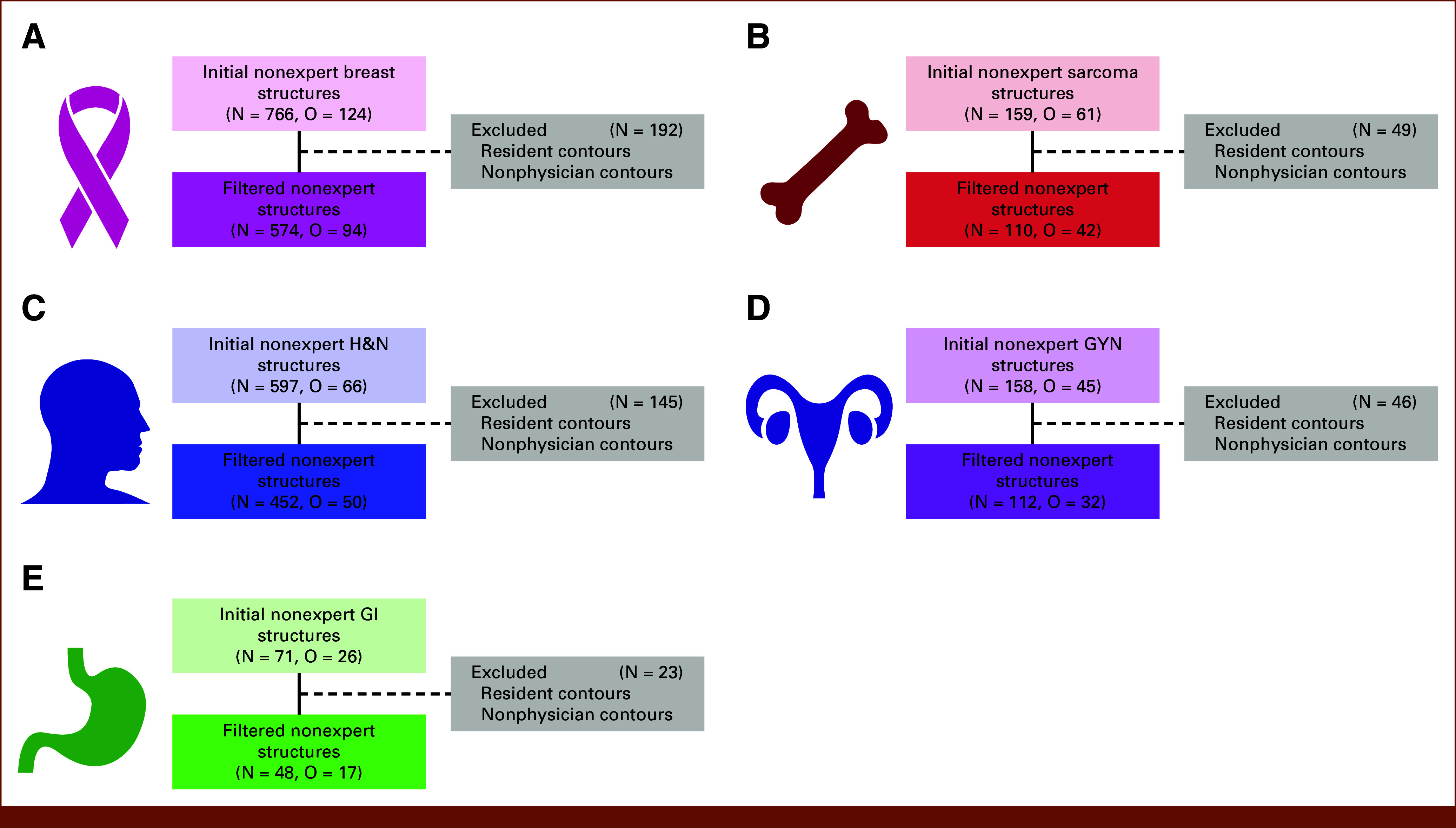
Methods: Organ at risk (OAR) and tumor-related segmentations provided by radiation oncologists from the Contouring Collaborative for Consensus in Radiation Oncology data set were used. Segmentations were derived from five disease sites: breast, sarcoma, head and neck (H&N), gynecologic (GYN), and GI. Segmentation quality was determined on a structure-by-structure basis by comparing the observer segmentations with an expert-derived consensus, which served as a reference standard benchmark. The Dice similarity coefficient (DSC) was primarily used as a metric for the comparisons. DSC was stratified into binary groups on the basis of structure-specific expert-derived interobserver variability (IOV) cutoffs. Generalized linear mixed-effects models using Bayesian estimation were used to investigate the association between demographic variables and the binarized DSC for each disease site. Variables with a highest density interval excluding zero were considered to substantially affect the outcome measure.
Results: Five hundred seventy-four, 110, 452, 112, and 48 segmentations were used for the breast, sarcoma, H&N, GYN, and GI cases, respectively. The median percentage of segmentations that crossed the expert DSC IOV cutoff when stratified by structure type was 55% and 31% for OARs and tumors, respectively. Regression analysis revealed that the structure being tumor-related had a substantial negative impact on binarized DSC for the breast, sarcoma, H&N, and GI cases. There were no recurring relationships between segmentation quality and demographic variables across the cases, with most variables demonstrating large standard deviations.
Conclusion: Our study highlights substantial uncertainty surrounding conventionally presumed factors influencing segmentation quality relative to benchmarks.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
