Ning Zhao, Yong Zhao, Mingze Chang, Gejuan Zhang, Ying Lu, Shilin Li, Juan Ma, QianQian Qi
{"title":"病例报告:孤立性眩晕是对侧水痘-带状疱疹病毒感染后左侧延髓梗死的唯一表现。","authors":"Ning Zhao, Yong Zhao, Mingze Chang, Gejuan Zhang, Ying Lu, Shilin Li, Juan Ma, QianQian Qi","doi":"10.1177/11795476241262213","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cerebral infarct associated with varicella-zoster virus (VZV) has been reported in the literature, while isolated central dizziness due to lateral medullary infarct (LMI) following VZV infection is rarely reported.</p><p><strong>Case report: </strong>We report the case of a 65-year-old man who presented to the neurology department because of herpes zoster on the right trigeminal nerve distribution. At 12 hours after admission, he developed transient vertigo along with nausea and unsteady walking and left-sided spontaneous horizontal nystagmus, gaze-evoked nystagmus, and upbeat nystagmus. The other usual signs of LMI including Horner syndrome, dysarthria, swallowing difficulty, and hemibody sensory change were absent. Video head impulse indicated decreased head impulse gain of the vestibulo-ocular reflex for the bilateral horizontal, anterior, and posterior semicircular canals with abnormal saccade waves. Suppression head impulse paradigm showed few downward saccades reflecting anti-compensatory saccades after the end of the head impulse back to the head-fixed target and decreased vestibulo-ocular reflex gain values of bilateral semicircular canals. Brain magnetic resonance imaging (MRI) showed a small infarct in the far dorsolateral portion of the left rostral medulla. The cerebrospinal fluid was positive for VZV DNA.</p><p><strong>Conclusions: </strong>In patients with VZV infection who develop dizziness, the possibility of cerebral infarct should be considered. Patients with facial herpes zoster and neurological symptoms always be screened for stroke using MRI and lumbar puncture should be performed and acyclovir administered empirically.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"17 ","pages":"11795476241262213"},"PeriodicalIF":0.6000,"publicationDate":"2024-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11185004/pdf/","citationCount":"0","resultStr":"{\"title\":\"Case Report: Isolated Vertigo as the Sole Manifestation of Left Lateral Medullary Infarction Following Contralateral Varicella-Zoster Virus Infection.\",\"authors\":\"Ning Zhao, Yong Zhao, Mingze Chang, Gejuan Zhang, Ying Lu, Shilin Li, Juan Ma, QianQian Qi\",\"doi\":\"10.1177/11795476241262213\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cerebral infarct associated with varicella-zoster virus (VZV) has been reported in the literature, while isolated central dizziness due to lateral medullary infarct (LMI) following VZV infection is rarely reported.</p><p><strong>Case report: </strong>We report the case of a 65-year-old man who presented to the neurology department because of herpes zoster on the right trigeminal nerve distribution. At 12 hours after admission, he developed transient vertigo along with nausea and unsteady walking and left-sided spontaneous horizontal nystagmus, gaze-evoked nystagmus, and upbeat nystagmus. The other usual signs of LMI including Horner syndrome, dysarthria, swallowing difficulty, and hemibody sensory change were absent. Video head impulse indicated decreased head impulse gain of the vestibulo-ocular reflex for the bilateral horizontal, anterior, and posterior semicircular canals with abnormal saccade waves. Suppression head impulse paradigm showed few downward saccades reflecting anti-compensatory saccades after the end of the head impulse back to the head-fixed target and decreased vestibulo-ocular reflex gain values of bilateral semicircular canals. Brain magnetic resonance imaging (MRI) showed a small infarct in the far dorsolateral portion of the left rostral medulla. The cerebrospinal fluid was positive for VZV DNA.</p><p><strong>Conclusions: </strong>In patients with VZV infection who develop dizziness, the possibility of cerebral infarct should be considered. Patients with facial herpes zoster and neurological symptoms always be screened for stroke using MRI and lumbar puncture should be performed and acyclovir administered empirically.</p>\",\"PeriodicalId\":10357,\"journal\":{\"name\":\"Clinical Medicine Insights. Case Reports\",\"volume\":\"17 \",\"pages\":\"11795476241262213\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2024-06-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11185004/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795476241262213\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476241262213","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Case Report: Isolated Vertigo as the Sole Manifestation of Left Lateral Medullary Infarction Following Contralateral Varicella-Zoster Virus Infection.
Background: Cerebral infarct associated with varicella-zoster virus (VZV) has been reported in the literature, while isolated central dizziness due to lateral medullary infarct (LMI) following VZV infection is rarely reported.
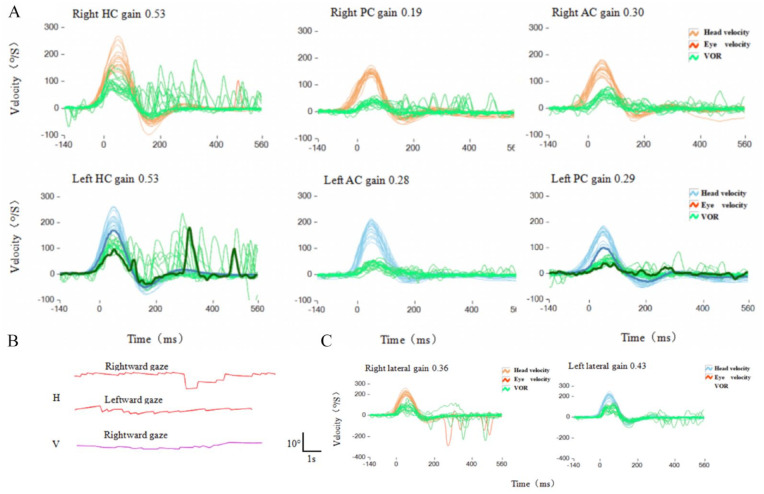
Case report: We report the case of a 65-year-old man who presented to the neurology department because of herpes zoster on the right trigeminal nerve distribution. At 12 hours after admission, he developed transient vertigo along with nausea and unsteady walking and left-sided spontaneous horizontal nystagmus, gaze-evoked nystagmus, and upbeat nystagmus. The other usual signs of LMI including Horner syndrome, dysarthria, swallowing difficulty, and hemibody sensory change were absent. Video head impulse indicated decreased head impulse gain of the vestibulo-ocular reflex for the bilateral horizontal, anterior, and posterior semicircular canals with abnormal saccade waves. Suppression head impulse paradigm showed few downward saccades reflecting anti-compensatory saccades after the end of the head impulse back to the head-fixed target and decreased vestibulo-ocular reflex gain values of bilateral semicircular canals. Brain magnetic resonance imaging (MRI) showed a small infarct in the far dorsolateral portion of the left rostral medulla. The cerebrospinal fluid was positive for VZV DNA.
Conclusions: In patients with VZV infection who develop dizziness, the possibility of cerebral infarct should be considered. Patients with facial herpes zoster and neurological symptoms always be screened for stroke using MRI and lumbar puncture should be performed and acyclovir administered empirically.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
