{"title":"医疗补助扩展与 30 天再入院:一项全国性研究。","authors":"Sami Tahhan MD, Cynthia Avila MBS, Chloe Carr MD, Rehan Qayyum MD, MHS","doi":"10.1002/jhm.13427","DOIUrl":null,"url":null,"abstract":"<p>In 2010, Congress enacted the Patient Protection and Affordable Care Act (ACA) to enhance health insurance affordability via subsidies and Medicaid expansion (ME). However, not all states adopted ME. We examined national hospital readmissions from 2005 to 2019 to investigate readmission reduction trends based on state ME status. The states were divided into those that expanded Medicaid in 2014 (ME-States) and those that did not until 2019 (non-ME States). Using a difference-in-difference framework and adjusting for hospital and population characteristics, we assessed the relationship between ME and 30-day readmissions following pneumonia, heart failure (HF), and acute myocardial infarction (AMI) hospitalizations. Both before and after the expansion, ME-States had higher mean readmission rates than non-ME-States. After ME, hospitals in ME-States exhibited larger reductions in readmission rates compared to non-ACA States: pneumonia (−0.12%; 95% confidence interval [CI] = −0.19%, −0.04%; <i>p</i> = .002), HF (−0.18%; 95% CI = −0.28%, −0.08%; <i>p</i> = .001), and AMI (−0.23%; 95% CI = −0.32%, −0.13%; <i>p</i> < .001).</p>","PeriodicalId":15883,"journal":{"name":"Journal of hospital medicine","volume":"19 10","pages":"924-928"},"PeriodicalIF":1.8000,"publicationDate":"2024-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhm.13427","citationCount":"0","resultStr":"{\"title\":\"Medicaid expansion and 30-day hospital readmissions: A nationwide study\",\"authors\":\"Sami Tahhan MD, Cynthia Avila MBS, Chloe Carr MD, Rehan Qayyum MD, MHS\",\"doi\":\"10.1002/jhm.13427\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In 2010, Congress enacted the Patient Protection and Affordable Care Act (ACA) to enhance health insurance affordability via subsidies and Medicaid expansion (ME). However, not all states adopted ME. We examined national hospital readmissions from 2005 to 2019 to investigate readmission reduction trends based on state ME status. The states were divided into those that expanded Medicaid in 2014 (ME-States) and those that did not until 2019 (non-ME States). Using a difference-in-difference framework and adjusting for hospital and population characteristics, we assessed the relationship between ME and 30-day readmissions following pneumonia, heart failure (HF), and acute myocardial infarction (AMI) hospitalizations. Both before and after the expansion, ME-States had higher mean readmission rates than non-ME-States. After ME, hospitals in ME-States exhibited larger reductions in readmission rates compared to non-ACA States: pneumonia (−0.12%; 95% confidence interval [CI] = −0.19%, −0.04%; <i>p</i> = .002), HF (−0.18%; 95% CI = −0.28%, −0.08%; <i>p</i> = .001), and AMI (−0.23%; 95% CI = −0.32%, −0.13%; <i>p</i> < .001).</p>\",\"PeriodicalId\":15883,\"journal\":{\"name\":\"Journal of hospital medicine\",\"volume\":\"19 10\",\"pages\":\"924-928\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-06-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhm.13427\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hospital medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.13427\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hospital medicine","FirstCategoryId":"3","ListUrlMain":"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.13427","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Medicaid expansion and 30-day hospital readmissions: A nationwide study
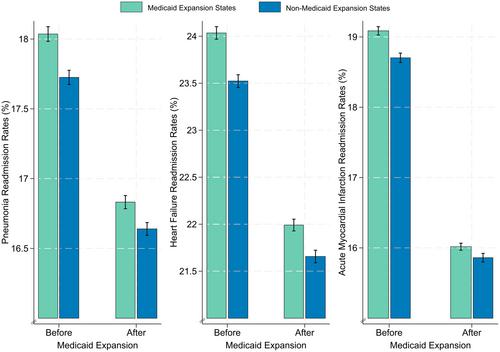
In 2010, Congress enacted the Patient Protection and Affordable Care Act (ACA) to enhance health insurance affordability via subsidies and Medicaid expansion (ME). However, not all states adopted ME. We examined national hospital readmissions from 2005 to 2019 to investigate readmission reduction trends based on state ME status. The states were divided into those that expanded Medicaid in 2014 (ME-States) and those that did not until 2019 (non-ME States). Using a difference-in-difference framework and adjusting for hospital and population characteristics, we assessed the relationship between ME and 30-day readmissions following pneumonia, heart failure (HF), and acute myocardial infarction (AMI) hospitalizations. Both before and after the expansion, ME-States had higher mean readmission rates than non-ME-States. After ME, hospitals in ME-States exhibited larger reductions in readmission rates compared to non-ACA States: pneumonia (−0.12%; 95% confidence interval [CI] = −0.19%, −0.04%; p = .002), HF (−0.18%; 95% CI = −0.28%, −0.08%; p = .001), and AMI (−0.23%; 95% CI = −0.32%, −0.13%; p < .001).
期刊介绍:
JHM is a peer-reviewed publication of the Society of Hospital Medicine and is published 12 times per year. JHM publishes manuscripts that address the care of hospitalized adults or children.
Broad areas of interest include (1) Treatments for common inpatient conditions; (2) Approaches to improving perioperative care; (3) Improving care for hospitalized patients with geriatric or pediatric vulnerabilities (such as mobility problems, or those with complex longitudinal care); (4) Evaluation of innovative healthcare delivery or educational models; (5) Approaches to improving the quality, safety, and value of healthcare across the acute- and postacute-continuum of care; and (6) Evaluation of policy and payment changes that affect hospital and postacute care.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
