{"title":"使用苯肾上腺素收缩血管可增加前负荷依赖型患者的心输出量。","authors":"Jakob Højlund, Mirjana Cihoric, Nicolai Bang Foss","doi":"10.1007/s10877-024-01186-7","DOIUrl":null,"url":null,"abstract":"<p><p>General Anaesthesia (GA) is accompanied by a marked decrease in sympathetic outflow and thus loss of vasomotor control of cardiac preload. The use of vasoconstriction during GA has mainly focused on maintaining blood pressure. Phenylephrine (PE) is a pure α1-agonist without inotropic effects widely used to correct intraoperative hypotension. The potential of PE for augmenting cardiac stroke volume (SV) and -output (CO) by venous recruitment is controversial and no human studies have explored the effects of PE in preload dependent circulation using indicator dilution technique. We hypothesized that PE-infusion in patients with cardiac stroke volume limited by reduced preload would restore preload and thus augment SV and CO. 20 patients undergoing GA for gastrointestinal surgery were monitored with arterial catheter and LiDCO unity monitor. Upon stable haemodynamics after induction patients were placed in head-up tilt (HUT). All patients became preload responsive as verified by a stroke volume variation (SVV) of > 12%. PE-infusion was then started at 15-20mikrg/min and adjusted until preload was restored (SVV < 12%). Li-dilution cardiac output (CO) was initially measured after induction (baseline), again with HUT in the preload responsive phase, and finally when preload was restored with infusion of PE.At baseline SVV was 10 ± 3% (mean ± st.dev.), CI was 2,6 ± 0,4 L/min*m<sup>2</sup>, and SVI 43 ± 7mL/m<sup>2</sup>. With HUT SVV was 19 ± 4%, CI was 2,2 ± 0,4 L/min*m<sup>2</sup>, SVI 35 ± 7mL/m<sup>2</sup>. During PE-infusion SVV was reduced to 6 ± 3%, CI increased to 2,6 ± 0,5 L/min*m<sup>2</sup>, and SVI increased to 49 ± 11mL/m<sup>2</sup>. All differences p < 0,001. In conclusion: Infusion of phenylephrine during preload dependency increased venous return abolishing preload dependency as evaluated by SVV and increased cardiac stroke volume and -output as measured by indicator-dilution technique. (ClinicalTrials.gov NCT05193097).</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"997-1002"},"PeriodicalIF":2.6000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11427527/pdf/","citationCount":"0","resultStr":"{\"title\":\"Vasoconstriction with phenylephrine increases cardiac output in preload dependent patients.\",\"authors\":\"Jakob Højlund, Mirjana Cihoric, Nicolai Bang Foss\",\"doi\":\"10.1007/s10877-024-01186-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>General Anaesthesia (GA) is accompanied by a marked decrease in sympathetic outflow and thus loss of vasomotor control of cardiac preload. The use of vasoconstriction during GA has mainly focused on maintaining blood pressure. Phenylephrine (PE) is a pure α1-agonist without inotropic effects widely used to correct intraoperative hypotension. The potential of PE for augmenting cardiac stroke volume (SV) and -output (CO) by venous recruitment is controversial and no human studies have explored the effects of PE in preload dependent circulation using indicator dilution technique. We hypothesized that PE-infusion in patients with cardiac stroke volume limited by reduced preload would restore preload and thus augment SV and CO. 20 patients undergoing GA for gastrointestinal surgery were monitored with arterial catheter and LiDCO unity monitor. Upon stable haemodynamics after induction patients were placed in head-up tilt (HUT). All patients became preload responsive as verified by a stroke volume variation (SVV) of > 12%. PE-infusion was then started at 15-20mikrg/min and adjusted until preload was restored (SVV < 12%). Li-dilution cardiac output (CO) was initially measured after induction (baseline), again with HUT in the preload responsive phase, and finally when preload was restored with infusion of PE.At baseline SVV was 10 ± 3% (mean ± st.dev.), CI was 2,6 ± 0,4 L/min*m<sup>2</sup>, and SVI 43 ± 7mL/m<sup>2</sup>. With HUT SVV was 19 ± 4%, CI was 2,2 ± 0,4 L/min*m<sup>2</sup>, SVI 35 ± 7mL/m<sup>2</sup>. During PE-infusion SVV was reduced to 6 ± 3%, CI increased to 2,6 ± 0,5 L/min*m<sup>2</sup>, and SVI increased to 49 ± 11mL/m<sup>2</sup>. All differences p < 0,001. In conclusion: Infusion of phenylephrine during preload dependency increased venous return abolishing preload dependency as evaluated by SVV and increased cardiac stroke volume and -output as measured by indicator-dilution technique. (ClinicalTrials.gov NCT05193097).</p>\",\"PeriodicalId\":15513,\"journal\":{\"name\":\"Journal of Clinical Monitoring and Computing\",\"volume\":\" \",\"pages\":\"997-1002\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11427527/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Monitoring and Computing\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10877-024-01186-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01186-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Vasoconstriction with phenylephrine increases cardiac output in preload dependent patients.
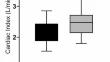
General Anaesthesia (GA) is accompanied by a marked decrease in sympathetic outflow and thus loss of vasomotor control of cardiac preload. The use of vasoconstriction during GA has mainly focused on maintaining blood pressure. Phenylephrine (PE) is a pure α1-agonist without inotropic effects widely used to correct intraoperative hypotension. The potential of PE for augmenting cardiac stroke volume (SV) and -output (CO) by venous recruitment is controversial and no human studies have explored the effects of PE in preload dependent circulation using indicator dilution technique. We hypothesized that PE-infusion in patients with cardiac stroke volume limited by reduced preload would restore preload and thus augment SV and CO. 20 patients undergoing GA for gastrointestinal surgery were monitored with arterial catheter and LiDCO unity monitor. Upon stable haemodynamics after induction patients were placed in head-up tilt (HUT). All patients became preload responsive as verified by a stroke volume variation (SVV) of > 12%. PE-infusion was then started at 15-20mikrg/min and adjusted until preload was restored (SVV < 12%). Li-dilution cardiac output (CO) was initially measured after induction (baseline), again with HUT in the preload responsive phase, and finally when preload was restored with infusion of PE.At baseline SVV was 10 ± 3% (mean ± st.dev.), CI was 2,6 ± 0,4 L/min*m2, and SVI 43 ± 7mL/m2. With HUT SVV was 19 ± 4%, CI was 2,2 ± 0,4 L/min*m2, SVI 35 ± 7mL/m2. During PE-infusion SVV was reduced to 6 ± 3%, CI increased to 2,6 ± 0,5 L/min*m2, and SVI increased to 49 ± 11mL/m2. All differences p < 0,001. In conclusion: Infusion of phenylephrine during preload dependency increased venous return abolishing preload dependency as evaluated by SVV and increased cardiac stroke volume and -output as measured by indicator-dilution technique. (ClinicalTrials.gov NCT05193097).
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
