Arvid Engström, Jonas Söderling, Anders Hviid, Björn Eliasson, Soffia Gudbjörnsdottir, Viktor Wintzell, Kristian Hveem, Christian Jonasson, Mads Melbye, Björn Pasternak, Peter Ueda
{"title":"安帕格列净和达帕格列净对心血管和肾脏疗效的比较:斯堪的纳维亚队列研究。","authors":"Arvid Engström, Jonas Söderling, Anders Hviid, Björn Eliasson, Soffia Gudbjörnsdottir, Viktor Wintzell, Kristian Hveem, Christian Jonasson, Mads Melbye, Björn Pasternak, Peter Ueda","doi":"10.1093/ehjcvp/pvae045","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>To assess the comparative cardiovascular and renal effectiveness and safety of empagliflozin vs. dapagliflozin among patients with type 2 diabetes in routine clinical practice.</p><p><strong>Methods and results: </strong>Cohort study using data from nationwide registers in Sweden, Denmark, and Norway, from June 2014 to June 2021 included 141 065 new users of empagliflozin and 58 306 new users of dapagliflozin. Coprimary outcomes were major cardiovascular events (myocardial infarction, stroke, and cardiovascular death), heart failure (hospitalization or death because of heart failure) and serious renal events (renal replacement therapy, hospitalization for renal events, and death from renal causes). Secondary outcomes were the individual components of the primary outcomes, any cause death, and diabetic ketoacidosis. Use of empagliflozin vs. dapagliflozin was associated with similar risk of major cardiovascular events [adjusted incidence rate: 15.9 vs. 15.8 events per 1000 person-years; HR 1.02, (95% confidence interval 0.97-1.08)], heart failure [6.5 vs. 6.3 events per 1000 person-years; HR 1.05 (0.97-1.14)] and serious renal events [3.7 vs. 4.1 events per 1000 person-years; HR 0.97 (0.87-1.07)]. In secondary outcome analyses, the HRs for use of empagliflozin vs. dapagliflozin were 1.00 (0.93-1.07) for myocardial infarction, 1.03 (0.95-1.12) for stroke, 1.01 (0.92-1.13) for cardiovascular death, 1.06 (1.00-1.11) for any cause death, 0.77 (0.60-0.99) for renal replacement therapy, 1.20 (0.75-1.93) for renal death, 1.01 (0.90-1.12) for hospitalization for renal events and 1.12 (0.94-1.33) for diabetic ketoacidosis.</p><p><strong>Conclusion: </strong>Use of empagliflozin and dapagliflozin was associated with similar risk of cardiovascular and renal outcomes, mortality, and diabetic ketoacidosis.</p>","PeriodicalId":11982,"journal":{"name":"European Heart Journal - Cardiovascular Pharmacotherapy","volume":" ","pages":"432-443"},"PeriodicalIF":6.1000,"publicationDate":"2024-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11411209/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative cardiovascular and renal effectiveness of empagliflozin and dapagliflozin: Scandinavian cohort study.\",\"authors\":\"Arvid Engström, Jonas Söderling, Anders Hviid, Björn Eliasson, Soffia Gudbjörnsdottir, Viktor Wintzell, Kristian Hveem, Christian Jonasson, Mads Melbye, Björn Pasternak, Peter Ueda\",\"doi\":\"10.1093/ehjcvp/pvae045\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>To assess the comparative cardiovascular and renal effectiveness and safety of empagliflozin vs. dapagliflozin among patients with type 2 diabetes in routine clinical practice.</p><p><strong>Methods and results: </strong>Cohort study using data from nationwide registers in Sweden, Denmark, and Norway, from June 2014 to June 2021 included 141 065 new users of empagliflozin and 58 306 new users of dapagliflozin. Coprimary outcomes were major cardiovascular events (myocardial infarction, stroke, and cardiovascular death), heart failure (hospitalization or death because of heart failure) and serious renal events (renal replacement therapy, hospitalization for renal events, and death from renal causes). Secondary outcomes were the individual components of the primary outcomes, any cause death, and diabetic ketoacidosis. Use of empagliflozin vs. dapagliflozin was associated with similar risk of major cardiovascular events [adjusted incidence rate: 15.9 vs. 15.8 events per 1000 person-years; HR 1.02, (95% confidence interval 0.97-1.08)], heart failure [6.5 vs. 6.3 events per 1000 person-years; HR 1.05 (0.97-1.14)] and serious renal events [3.7 vs. 4.1 events per 1000 person-years; HR 0.97 (0.87-1.07)]. In secondary outcome analyses, the HRs for use of empagliflozin vs. dapagliflozin were 1.00 (0.93-1.07) for myocardial infarction, 1.03 (0.95-1.12) for stroke, 1.01 (0.92-1.13) for cardiovascular death, 1.06 (1.00-1.11) for any cause death, 0.77 (0.60-0.99) for renal replacement therapy, 1.20 (0.75-1.93) for renal death, 1.01 (0.90-1.12) for hospitalization for renal events and 1.12 (0.94-1.33) for diabetic ketoacidosis.</p><p><strong>Conclusion: </strong>Use of empagliflozin and dapagliflozin was associated with similar risk of cardiovascular and renal outcomes, mortality, and diabetic ketoacidosis.</p>\",\"PeriodicalId\":11982,\"journal\":{\"name\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"volume\":\" \",\"pages\":\"432-443\"},\"PeriodicalIF\":6.1000,\"publicationDate\":\"2024-08-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11411209/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjcvp/pvae045\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvae045","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:在常规临床实践中,评估恩格列净与达帕格列净对2型糖尿病患者心血管和肾脏有效性和安全性的比较:队列研究使用瑞典、丹麦和挪威2014年6月至2021年6月期间全国范围内的登记数据,包括141065名安帕格列净新用户和58306名达帕格列净新用户。主要结果为重大心血管事件(心肌梗死、中风和心血管死亡)、心力衰竭(因心力衰竭住院或死亡)和严重肾脏事件(肾脏替代治疗、因肾脏事件住院和因肾脏原因死亡)。次要结果为主要结果的各个组成部分、任何原因导致的死亡和糖尿病酮症酸中毒:结果:使用empagliflozin与使用dapagliflozin发生重大心血管事件的风险相似(调整后发病率分别为15.9%和15.8%):15.9 vs. 15.8次/1000人-年;HR 1.02 [95% CI 0.97-1.08])、心力衰竭(6.5 vs. 6.3次/1000人-年;HR 1.05 [0.97-1.14])和严重肾脏事件(3.7 vs. 4.1次/1000人-年;HR 0.97 [0.87-1.07])的风险相似。在次要结局分析中,使用empagliflozin与dapagliflozin相比,心肌梗死的HR为1.00(0.93-1.07),中风为1.03(0.95-1.12),心血管死亡为1.01(0.92-1.13),任何原因死亡为1.06(1.00-1.11)、肾脏替代治疗0.77(0.60-0.99)、肾脏死亡1.20(0.75-1.93)、肾脏事件住院1.01(0.90-1.12)、糖尿病酮症酸中毒1.12(0.94-1.33):使用empagliflozin和dapagliflozin与心血管和肾脏结局、死亡率和糖尿病酮症酸中毒的风险相似。
Comparative cardiovascular and renal effectiveness of empagliflozin and dapagliflozin: Scandinavian cohort study.
Aims: To assess the comparative cardiovascular and renal effectiveness and safety of empagliflozin vs. dapagliflozin among patients with type 2 diabetes in routine clinical practice.
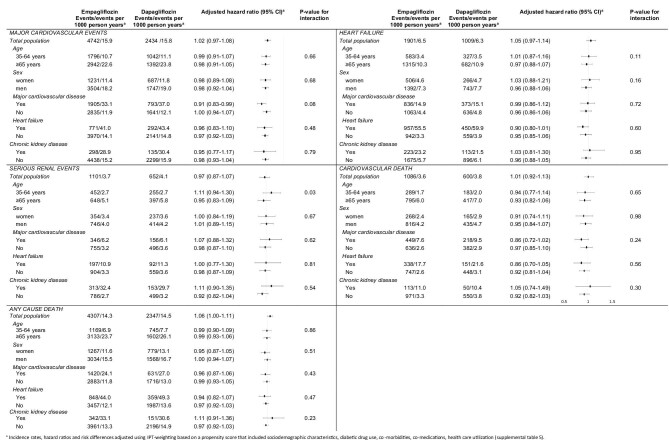
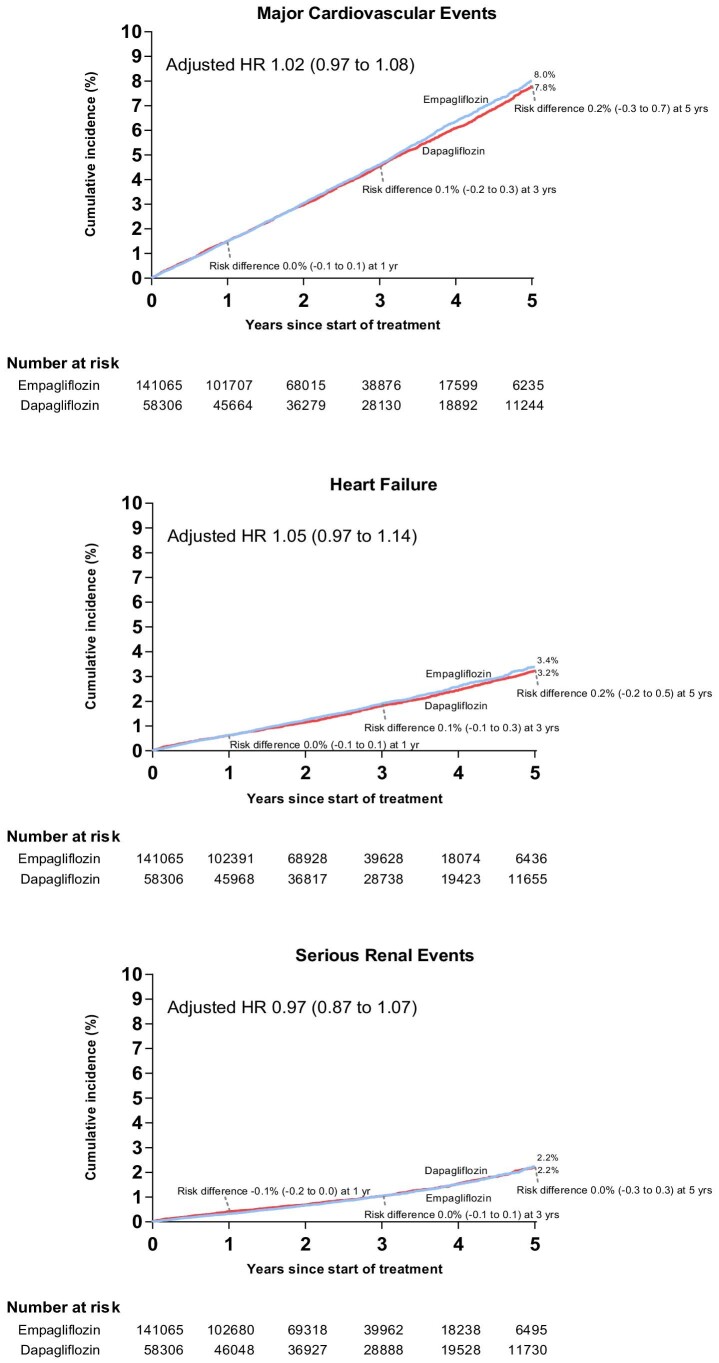
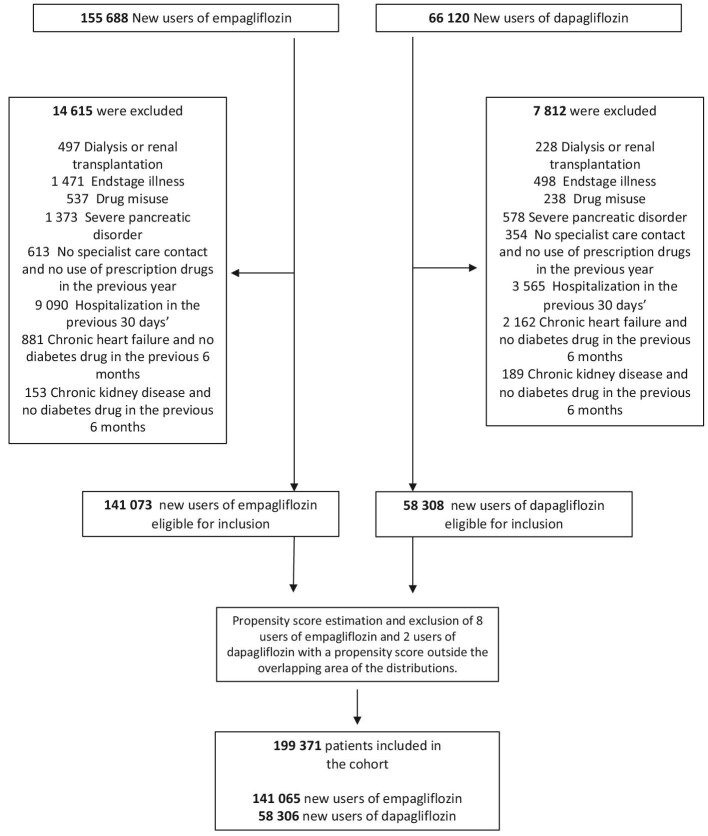
Methods and results: Cohort study using data from nationwide registers in Sweden, Denmark, and Norway, from June 2014 to June 2021 included 141 065 new users of empagliflozin and 58 306 new users of dapagliflozin. Coprimary outcomes were major cardiovascular events (myocardial infarction, stroke, and cardiovascular death), heart failure (hospitalization or death because of heart failure) and serious renal events (renal replacement therapy, hospitalization for renal events, and death from renal causes). Secondary outcomes were the individual components of the primary outcomes, any cause death, and diabetic ketoacidosis. Use of empagliflozin vs. dapagliflozin was associated with similar risk of major cardiovascular events [adjusted incidence rate: 15.9 vs. 15.8 events per 1000 person-years; HR 1.02, (95% confidence interval 0.97-1.08)], heart failure [6.5 vs. 6.3 events per 1000 person-years; HR 1.05 (0.97-1.14)] and serious renal events [3.7 vs. 4.1 events per 1000 person-years; HR 0.97 (0.87-1.07)]. In secondary outcome analyses, the HRs for use of empagliflozin vs. dapagliflozin were 1.00 (0.93-1.07) for myocardial infarction, 1.03 (0.95-1.12) for stroke, 1.01 (0.92-1.13) for cardiovascular death, 1.06 (1.00-1.11) for any cause death, 0.77 (0.60-0.99) for renal replacement therapy, 1.20 (0.75-1.93) for renal death, 1.01 (0.90-1.12) for hospitalization for renal events and 1.12 (0.94-1.33) for diabetic ketoacidosis.
Conclusion: Use of empagliflozin and dapagliflozin was associated with similar risk of cardiovascular and renal outcomes, mortality, and diabetic ketoacidosis.
期刊介绍:
The European Heart Journal - Cardiovascular Pharmacotherapy (EHJ-CVP) is an international, peer-reviewed journal published in English, specifically dedicated to clinical cardiovascular pharmacology. EHJ-CVP publishes original articles focusing on clinical research involving both new and established drugs and methods, along with meta-analyses and topical reviews. The journal's primary aim is to enhance the pharmacological treatment of patients with cardiovascular disease by interpreting and integrating new scientific developments in this field.
While the emphasis is on clinical topics, EHJ-CVP also considers basic research articles from fields such as physiology and molecular biology that contribute to the understanding of cardiovascular drug therapy. These may include articles related to new drug development and evaluation, the physiological and pharmacological basis of drug action, metabolism, drug interactions, and side effects.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
