Andrew Sharp, Christine Cornforth, Richard Jackson, Jane Harrold, Mark A. Turner, Louise C. Kenny, Philip N. Baker, Edward D. Johnstone, Asma Khalil, Peter von Dadelszen, Aris T. Papageorghiou, Zarko Alfirevic, Brigitte Vollmer, the STRIDER group
{"title":"宫内接受西地那非治疗的儿童 2 岁时的神经发育结果:STRIDER随机对照试验。","authors":"Andrew Sharp, Christine Cornforth, Richard Jackson, Jane Harrold, Mark A. Turner, Louise C. Kenny, Philip N. Baker, Edward D. Johnstone, Asma Khalil, Peter von Dadelszen, Aris T. Papageorghiou, Zarko Alfirevic, Brigitte Vollmer, the STRIDER group","doi":"10.1111/1471-0528.17888","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>Severe early-onset fetal growth restriction (FGR) causes stillbirth, neonatal death and neurodevelopmental impairment. Poor maternal spiral artery remodelling maintains vasoactive responsiveness but is susceptible to treatment with sildenafil, a phosphodiesterase type 5 (PDE5) inhibitor, which may improve perinatal outcomes.</p>\n </section>\n \n <section>\n \n <h3> Design</h3>\n \n <p>Superiority, double-blind randomised controlled trial.</p>\n </section>\n \n <section>\n \n <h3> Setting</h3>\n \n <p>A total of 20 UK fetal medicine units.</p>\n </section>\n \n <section>\n \n <h3> Population</h3>\n \n <p>Pregnancies affected by FGR, defined as an abdominal circumference below the tenth centile with absent end-diastolic flow in the umbilical artery between 22<sup>+0</sup> and 29<sup>+6</sup> weeks of gestation.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Treatment with sildenafil (25 mg three times/day) or placebo until delivery or 32 weeks of gestation.</p>\n </section>\n \n <section>\n \n <h3> Main outcome measures</h3>\n \n <p>All infants alive at hospital discharge were assessed for cardiovascular function and cognitive, speech/language and neuromotor impairment at 2 years of age. The primary outcome was survival without cerebral palsy or neurosensory impairment, or a Bayley-III composite score of >85.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In total, 135 women were randomised between November 2014 and July 2016 (70 to sildenafil and 65 to placebo). We previously published that there was no improvement in time to delivery or perinatal outcomes with sildenafil. In all, 75 babies (55.5%) were discharged alive, with 61 infants eligible for follow-up (32 sildenafil and 29 placebo). One infant died (placebo), three mothers declined and ten mothers were uncontactable. There was no difference in neurodevelopment or blood pressure following treatment with sildenafil. Infants who received sildenafil had a larger head circumference at 2 years of age (median difference 49.2 cm, IQR 46.4–50.3, vs 47.2 cm, 95% CI 44.7–48.9 cm).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Sildenafil therapy did not prolong pregnancy or improve perinatal outcomes and did not improve infant neurodevelopment in FGR survivors. Therefore, sildenafil should not be prescribed for this condition.</p>\n </section>\n </div>","PeriodicalId":50729,"journal":{"name":"Bjog-An International Journal of Obstetrics and Gynaecology","volume":"131 12","pages":"1673-1683"},"PeriodicalIF":4.8000,"publicationDate":"2024-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1471-0528.17888","citationCount":"0","resultStr":"{\"title\":\"Neurodevelopmental outcomes at 2 years in children who received sildenafil therapy in utero: The STRIDER randomised controlled trial\",\"authors\":\"Andrew Sharp, Christine Cornforth, Richard Jackson, Jane Harrold, Mark A. Turner, Louise C. Kenny, Philip N. Baker, Edward D. Johnstone, Asma Khalil, Peter von Dadelszen, Aris T. Papageorghiou, Zarko Alfirevic, Brigitte Vollmer, the STRIDER group\",\"doi\":\"10.1111/1471-0528.17888\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>Severe early-onset fetal growth restriction (FGR) causes stillbirth, neonatal death and neurodevelopmental impairment. Poor maternal spiral artery remodelling maintains vasoactive responsiveness but is susceptible to treatment with sildenafil, a phosphodiesterase type 5 (PDE5) inhibitor, which may improve perinatal outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Design</h3>\\n \\n <p>Superiority, double-blind randomised controlled trial.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Setting</h3>\\n \\n <p>A total of 20 UK fetal medicine units.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Population</h3>\\n \\n <p>Pregnancies affected by FGR, defined as an abdominal circumference below the tenth centile with absent end-diastolic flow in the umbilical artery between 22<sup>+0</sup> and 29<sup>+6</sup> weeks of gestation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Treatment with sildenafil (25 mg three times/day) or placebo until delivery or 32 weeks of gestation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Main outcome measures</h3>\\n \\n <p>All infants alive at hospital discharge were assessed for cardiovascular function and cognitive, speech/language and neuromotor impairment at 2 years of age. The primary outcome was survival without cerebral palsy or neurosensory impairment, or a Bayley-III composite score of >85.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>In total, 135 women were randomised between November 2014 and July 2016 (70 to sildenafil and 65 to placebo). We previously published that there was no improvement in time to delivery or perinatal outcomes with sildenafil. In all, 75 babies (55.5%) were discharged alive, with 61 infants eligible for follow-up (32 sildenafil and 29 placebo). One infant died (placebo), three mothers declined and ten mothers were uncontactable. There was no difference in neurodevelopment or blood pressure following treatment with sildenafil. Infants who received sildenafil had a larger head circumference at 2 years of age (median difference 49.2 cm, IQR 46.4–50.3, vs 47.2 cm, 95% CI 44.7–48.9 cm).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Sildenafil therapy did not prolong pregnancy or improve perinatal outcomes and did not improve infant neurodevelopment in FGR survivors. Therefore, sildenafil should not be prescribed for this condition.</p>\\n </section>\\n </div>\",\"PeriodicalId\":50729,\"journal\":{\"name\":\"Bjog-An International Journal of Obstetrics and Gynaecology\",\"volume\":\"131 12\",\"pages\":\"1673-1683\"},\"PeriodicalIF\":4.8000,\"publicationDate\":\"2024-06-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1471-0528.17888\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bjog-An International Journal of Obstetrics and Gynaecology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.17888\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bjog-An International Journal of Obstetrics and Gynaecology","FirstCategoryId":"3","ListUrlMain":"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.17888","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Neurodevelopmental outcomes at 2 years in children who received sildenafil therapy in utero: The STRIDER randomised controlled trial
Objective
Severe early-onset fetal growth restriction (FGR) causes stillbirth, neonatal death and neurodevelopmental impairment. Poor maternal spiral artery remodelling maintains vasoactive responsiveness but is susceptible to treatment with sildenafil, a phosphodiesterase type 5 (PDE5) inhibitor, which may improve perinatal outcomes.
Pregnancies affected by FGR, defined as an abdominal circumference below the tenth centile with absent end-diastolic flow in the umbilical artery between 22+0 and 29+6 weeks of gestation.
Methods
Treatment with sildenafil (25 mg three times/day) or placebo until delivery or 32 weeks of gestation.
Main outcome measures
All infants alive at hospital discharge were assessed for cardiovascular function and cognitive, speech/language and neuromotor impairment at 2 years of age. The primary outcome was survival without cerebral palsy or neurosensory impairment, or a Bayley-III composite score of >85.
Results
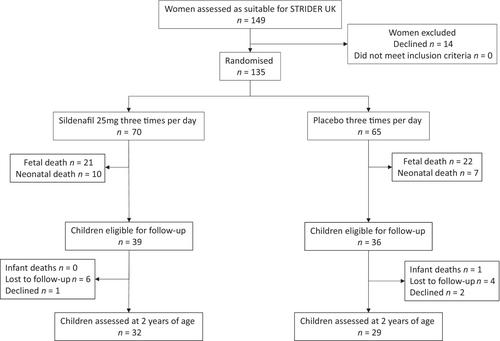
In total, 135 women were randomised between November 2014 and July 2016 (70 to sildenafil and 65 to placebo). We previously published that there was no improvement in time to delivery or perinatal outcomes with sildenafil. In all, 75 babies (55.5%) were discharged alive, with 61 infants eligible for follow-up (32 sildenafil and 29 placebo). One infant died (placebo), three mothers declined and ten mothers were uncontactable. There was no difference in neurodevelopment or blood pressure following treatment with sildenafil. Infants who received sildenafil had a larger head circumference at 2 years of age (median difference 49.2 cm, IQR 46.4–50.3, vs 47.2 cm, 95% CI 44.7–48.9 cm).
Conclusions
Sildenafil therapy did not prolong pregnancy or improve perinatal outcomes and did not improve infant neurodevelopment in FGR survivors. Therefore, sildenafil should not be prescribed for this condition.
期刊介绍:
BJOG is an editorially independent publication owned by the Royal College of Obstetricians and Gynaecologists (RCOG). The Journal publishes original, peer-reviewed work in all areas of obstetrics and gynaecology, including contraception, urogynaecology, fertility, oncology and clinical practice. Its aim is to publish the highest quality medical research in women''s health, worldwide.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
