{"title":"治疗 B 型主动脉夹层时支架移植物的最佳近端着床区是哪里?","authors":"Tomoki Cho, Keiji Uchida, Shota Yasuda, Ryo Izubuchi, Shotaro Kaneko, Tomoyuki Minami, Aya Saito","doi":"10.1007/s00270-024-03791-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Retrograde type A aortic dissection (RTAD) represents a serious complication of endovascular treatment for type B aortic dissection (TBAD). To avoid RTAD, it is recommended to land the proximal end of the stent graft in a non-dissected aortic segment. In this study, we investigated whether landing in the dissection area increased the number of events at the proximal site.</p><p><strong>Methods: </strong>We conducted a retrospective review of endovascular treatments for TBAD at a single institution between 2009 and 2022. Patients were divided into two groups: group A, with a proximal landing zone entirely within the dissected area, and group B, with the proximal extent of the seal zone in the non-dissected area. We evaluated the occurrence of proximal events, including RTAD, and examined long-term outcomes to assess the validity of landing in the dissection area.</p><p><strong>Results: </strong>The study included eighty-nine patients who underwent endovascular treatment for TBAD. New intimal tears in the proximal landing site occurred in 3 cases (3.4%), with 1 case (2%) in group A and 2 cases (5.1%) in group B, showing no significant difference. Among the three cases, one (1.1%) in group B with zone 2 landing resulted in RTAD. At 60 months, the overall survival was 85%, and freedom from aorta-related mortality was 88%, with no significant difference between the groups.</p><p><strong>Conclusion: </strong>Even if the proximal landing is in a dissected area, a treatment strategy performed in zone 3 without proximal landing in zone 2, seeking a non-dissected area, can still provide sufficient therapeutic effects. Level of Evidence 3 Retrospective single-center cohort analysis.</p>","PeriodicalId":9591,"journal":{"name":"CardioVascular and Interventional Radiology","volume":" ","pages":"1037-1044"},"PeriodicalIF":2.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"What is the Optimal Proximal Landing Zone of the Stent Graft in Treatment of Aortic Type B Dissection?\",\"authors\":\"Tomoki Cho, Keiji Uchida, Shota Yasuda, Ryo Izubuchi, Shotaro Kaneko, Tomoyuki Minami, Aya Saito\",\"doi\":\"10.1007/s00270-024-03791-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Retrograde type A aortic dissection (RTAD) represents a serious complication of endovascular treatment for type B aortic dissection (TBAD). To avoid RTAD, it is recommended to land the proximal end of the stent graft in a non-dissected aortic segment. In this study, we investigated whether landing in the dissection area increased the number of events at the proximal site.</p><p><strong>Methods: </strong>We conducted a retrospective review of endovascular treatments for TBAD at a single institution between 2009 and 2022. Patients were divided into two groups: group A, with a proximal landing zone entirely within the dissected area, and group B, with the proximal extent of the seal zone in the non-dissected area. We evaluated the occurrence of proximal events, including RTAD, and examined long-term outcomes to assess the validity of landing in the dissection area.</p><p><strong>Results: </strong>The study included eighty-nine patients who underwent endovascular treatment for TBAD. New intimal tears in the proximal landing site occurred in 3 cases (3.4%), with 1 case (2%) in group A and 2 cases (5.1%) in group B, showing no significant difference. Among the three cases, one (1.1%) in group B with zone 2 landing resulted in RTAD. At 60 months, the overall survival was 85%, and freedom from aorta-related mortality was 88%, with no significant difference between the groups.</p><p><strong>Conclusion: </strong>Even if the proximal landing is in a dissected area, a treatment strategy performed in zone 3 without proximal landing in zone 2, seeking a non-dissected area, can still provide sufficient therapeutic effects. Level of Evidence 3 Retrospective single-center cohort analysis.</p>\",\"PeriodicalId\":9591,\"journal\":{\"name\":\"CardioVascular and Interventional Radiology\",\"volume\":\" \",\"pages\":\"1037-1044\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CardioVascular and Interventional Radiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00270-024-03791-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CardioVascular and Interventional Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00270-024-03791-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
What is the Optimal Proximal Landing Zone of the Stent Graft in Treatment of Aortic Type B Dissection?
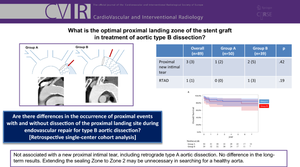
Purpose: Retrograde type A aortic dissection (RTAD) represents a serious complication of endovascular treatment for type B aortic dissection (TBAD). To avoid RTAD, it is recommended to land the proximal end of the stent graft in a non-dissected aortic segment. In this study, we investigated whether landing in the dissection area increased the number of events at the proximal site.
Methods: We conducted a retrospective review of endovascular treatments for TBAD at a single institution between 2009 and 2022. Patients were divided into two groups: group A, with a proximal landing zone entirely within the dissected area, and group B, with the proximal extent of the seal zone in the non-dissected area. We evaluated the occurrence of proximal events, including RTAD, and examined long-term outcomes to assess the validity of landing in the dissection area.
Results: The study included eighty-nine patients who underwent endovascular treatment for TBAD. New intimal tears in the proximal landing site occurred in 3 cases (3.4%), with 1 case (2%) in group A and 2 cases (5.1%) in group B, showing no significant difference. Among the three cases, one (1.1%) in group B with zone 2 landing resulted in RTAD. At 60 months, the overall survival was 85%, and freedom from aorta-related mortality was 88%, with no significant difference between the groups.
Conclusion: Even if the proximal landing is in a dissected area, a treatment strategy performed in zone 3 without proximal landing in zone 2, seeking a non-dissected area, can still provide sufficient therapeutic effects. Level of Evidence 3 Retrospective single-center cohort analysis.
期刊介绍:
CardioVascular and Interventional Radiology (CVIR) is the official journal of the Cardiovascular and Interventional Radiological Society of Europe, and is also the official organ of a number of additional distinguished national and international interventional radiological societies. CVIR publishes double blinded peer-reviewed original research work including clinical and laboratory investigations, technical notes, case reports, works in progress, and letters to the editor, as well as review articles, pictorial essays, editorials, and special invited submissions in the field of vascular and interventional radiology. Beside the communication of the latest research results in this field, it is also the aim of CVIR to support continuous medical education. Articles that are accepted for publication are done so with the understanding that they, or their substantive contents, have not been and will not be submitted to any other publication.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
