Zhuxin Zhang, Le Li, Zhenhao Zhang, Zhao Hu, Yulong Xiong, Likun Zhou, Yan Yao
{"title":"高血压左心室肥厚的心电图追踪:SPRINT 试验的发病率和预后结果。","authors":"Zhuxin Zhang, Le Li, Zhenhao Zhang, Zhao Hu, Yulong Xiong, Likun Zhou, Yan Yao","doi":"10.1186/s40885-024-00275-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study explores the impact of intensive blood pressure (BP) control on left ventricular hypertrophy (LVH) incidence and evaluates the prognostic implications of LVH status (pre-existing/new-onset/persistent/regression) using Systolic Blood Pressure Intervention Trial (SPRINT) Electrocardiogram Data.</p><p><strong>Methods: </strong>Poisson regression was used to assess new-onset LVH and LVH regression rates. Multivariable-adjusted Cox proportional hazard models determined the risk of adverse cardiovascular events (ACE), a composite of myocardial infarction (MI), non-MI acute coronary syndrome, stroke, heart failure, or cardiovascular death, alongside safety adverse events.</p><p><strong>Results: </strong>In 8,016 participants, intensive BP control significantly reduced new-onset LVH (8.27 vs. 14.79 per 1000-person years; adjusted p<0.001) and increased LVH regression (14.89 vs. 11.89 per 1000-person years; adjusted p<0.001). Elevated ACE risk was notable in participants with pre-existing LVH [adjusted HR: 1.94 (95% CI: 1.25-2.99); p = 0.003], new-onset LVH [adjusted 1.74 (95% CI: 1.16-2.60); p = 0.007], and persistent LVH[adjusted HR: 1.96 (95% CI: 1.11-3.46); p = 0.020], compared to those without LVH. Intriguingly, LVH regression attenuated this risk increment [adjusted HR: 1.57 (95% CI: 0.98-2.53); p = 0.062]. Achieving a BP target of < 120/80 mmHg nullified the increased ACE risk in those with pre-existing LVH.</p><p><strong>Conclusions: </strong>Intensive BP control is instrumental in both reducing the emergence of LVH and fostering its regression. Pre-existing, new-onset LVH and persistent LV remain a predictor of adverse cardiovascular prognosis, whereas LVH regression and achieving on-treatment BP < 120/80 mmHg in pre-existing LVH individuals may further mitigate residual cardiovascular risk.</p><p><strong>Clinical trial registration: </strong>URL: ClinicalTrials.gov Unique Identifier: NCT01206062.</p>","PeriodicalId":10480,"journal":{"name":"Clinical Hypertension","volume":"30 1","pages":"17"},"PeriodicalIF":6.2000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11215828/pdf/","citationCount":"0","resultStr":"{\"title\":\"Electrocardiographic tracking of left ventricular hypertrophy in hypertension: incidence and prognostic outcomes from the SPRINT trial.\",\"authors\":\"Zhuxin Zhang, Le Li, Zhenhao Zhang, Zhao Hu, Yulong Xiong, Likun Zhou, Yan Yao\",\"doi\":\"10.1186/s40885-024-00275-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study explores the impact of intensive blood pressure (BP) control on left ventricular hypertrophy (LVH) incidence and evaluates the prognostic implications of LVH status (pre-existing/new-onset/persistent/regression) using Systolic Blood Pressure Intervention Trial (SPRINT) Electrocardiogram Data.</p><p><strong>Methods: </strong>Poisson regression was used to assess new-onset LVH and LVH regression rates. Multivariable-adjusted Cox proportional hazard models determined the risk of adverse cardiovascular events (ACE), a composite of myocardial infarction (MI), non-MI acute coronary syndrome, stroke, heart failure, or cardiovascular death, alongside safety adverse events.</p><p><strong>Results: </strong>In 8,016 participants, intensive BP control significantly reduced new-onset LVH (8.27 vs. 14.79 per 1000-person years; adjusted p<0.001) and increased LVH regression (14.89 vs. 11.89 per 1000-person years; adjusted p<0.001). Elevated ACE risk was notable in participants with pre-existing LVH [adjusted HR: 1.94 (95% CI: 1.25-2.99); p = 0.003], new-onset LVH [adjusted 1.74 (95% CI: 1.16-2.60); p = 0.007], and persistent LVH[adjusted HR: 1.96 (95% CI: 1.11-3.46); p = 0.020], compared to those without LVH. Intriguingly, LVH regression attenuated this risk increment [adjusted HR: 1.57 (95% CI: 0.98-2.53); p = 0.062]. Achieving a BP target of < 120/80 mmHg nullified the increased ACE risk in those with pre-existing LVH.</p><p><strong>Conclusions: </strong>Intensive BP control is instrumental in both reducing the emergence of LVH and fostering its regression. Pre-existing, new-onset LVH and persistent LV remain a predictor of adverse cardiovascular prognosis, whereas LVH regression and achieving on-treatment BP < 120/80 mmHg in pre-existing LVH individuals may further mitigate residual cardiovascular risk.</p><p><strong>Clinical trial registration: </strong>URL: ClinicalTrials.gov Unique Identifier: NCT01206062.</p>\",\"PeriodicalId\":10480,\"journal\":{\"name\":\"Clinical Hypertension\",\"volume\":\"30 1\",\"pages\":\"17\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11215828/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Hypertension\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40885-024-00275-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Hypertension","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40885-024-00275-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Electrocardiographic tracking of left ventricular hypertrophy in hypertension: incidence and prognostic outcomes from the SPRINT trial.
Background: This study explores the impact of intensive blood pressure (BP) control on left ventricular hypertrophy (LVH) incidence and evaluates the prognostic implications of LVH status (pre-existing/new-onset/persistent/regression) using Systolic Blood Pressure Intervention Trial (SPRINT) Electrocardiogram Data.
Methods: Poisson regression was used to assess new-onset LVH and LVH regression rates. Multivariable-adjusted Cox proportional hazard models determined the risk of adverse cardiovascular events (ACE), a composite of myocardial infarction (MI), non-MI acute coronary syndrome, stroke, heart failure, or cardiovascular death, alongside safety adverse events.
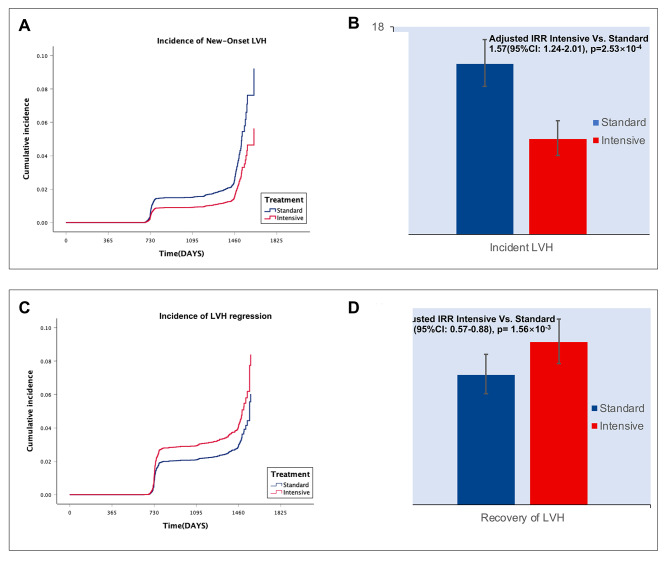
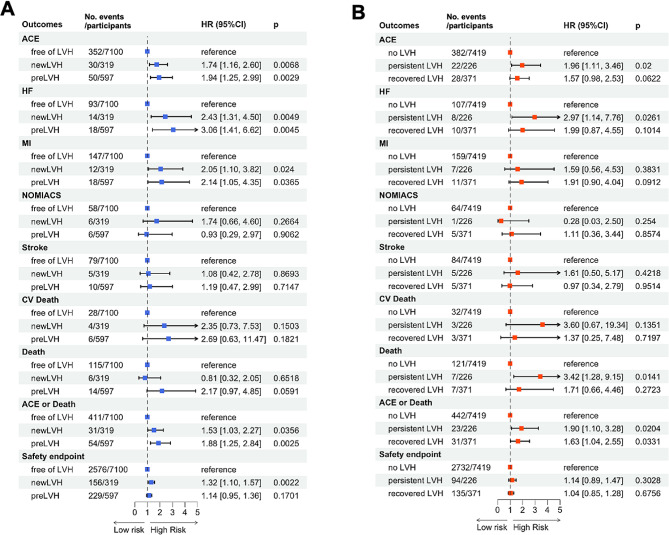
Results: In 8,016 participants, intensive BP control significantly reduced new-onset LVH (8.27 vs. 14.79 per 1000-person years; adjusted p<0.001) and increased LVH regression (14.89 vs. 11.89 per 1000-person years; adjusted p<0.001). Elevated ACE risk was notable in participants with pre-existing LVH [adjusted HR: 1.94 (95% CI: 1.25-2.99); p = 0.003], new-onset LVH [adjusted 1.74 (95% CI: 1.16-2.60); p = 0.007], and persistent LVH[adjusted HR: 1.96 (95% CI: 1.11-3.46); p = 0.020], compared to those without LVH. Intriguingly, LVH regression attenuated this risk increment [adjusted HR: 1.57 (95% CI: 0.98-2.53); p = 0.062]. Achieving a BP target of < 120/80 mmHg nullified the increased ACE risk in those with pre-existing LVH.
Conclusions: Intensive BP control is instrumental in both reducing the emergence of LVH and fostering its regression. Pre-existing, new-onset LVH and persistent LV remain a predictor of adverse cardiovascular prognosis, whereas LVH regression and achieving on-treatment BP < 120/80 mmHg in pre-existing LVH individuals may further mitigate residual cardiovascular risk.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
