Amandine Dernoncourt, Kaies Hedhli, Noémie Abisror, Meryam Cheloufi, Jonathan Cohen, Kamila Kolanska, Chloé McAvoy, Lise Selleret, Eric Ballot, Emmanuelle Mathieu d'Argent, Nathalie Chabbert Buffet, Olivier Fain, Gilles Kayem, Arsène Mekinian
{"title":"羟氯喹治疗复发性妊娠失败:来自法国前瞻性多中心登记处的数据。","authors":"Amandine Dernoncourt, Kaies Hedhli, Noémie Abisror, Meryam Cheloufi, Jonathan Cohen, Kamila Kolanska, Chloé McAvoy, Lise Selleret, Eric Ballot, Emmanuelle Mathieu d'Argent, Nathalie Chabbert Buffet, Olivier Fain, Gilles Kayem, Arsène Mekinian","doi":"10.1093/humrep/deae146","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>What are the outcomes of pregnancies exposed to hydroxychloroquine (HCQ) in women with a history of recurrent pregnancy loss (RPL), and what factors predict the course of these pregnancies beyond the first trimester?</p><p><strong>Summary answer: </strong>In our cohort of pregnancies in women with a history of RPL exposed to HCQ early in pregnancy, we found that the only factor determining the success of these pregnancies was the number of previous miscarriages.</p><p><strong>What is known already: </strong>Dysregulation of the maternal immune system plays a role in RPL. HCQ, with its dual immunomodulating and vascular protective effects, is a potential treatment for unexplained RPL.</p><p><strong>Study design, size, duration: </strong>The FALCO (Facteurs de récidive précoce des fausses couches) registry is an ongoing French multicenter infertility registry established in 2017 that includes women (aged from 18 to 49 years) with a history of spontaneous RPL (at least three early miscarriages (≤12 weeks of gestation (WG)) recruited from several university hospitals.</p><p><strong>Participants/materials, setting, methods: </strong>Spontaneous pregnancies enrolled in the FALCO registry with an exposure to HCQ (before conception or at the start of pregnancy) were included. Pregnancies concomitantly exposed to tumor necrosis factor inhibitors, interleukin-1 and -2 inhibitors, intravenous immunoglobulin, and/or intravenous intralipid infusion, were excluded. Concomitant treatment with low-dose aspirin (LDA), low-molecular weight heparin (LMWH), progesterone, and/or prednisone was allowed. All patients underwent the recommended evaluations for investigating RPL. Those who became pregnant received obstetric care in accordance with French recommendations and were followed prospectively. The main endpoint was the occurrence of a pregnancy continuing beyond 12 WG, and the secondary endpoint was the occurrence of a live birth.</p><p><strong>Main results and the role of chance: </strong>One hundred pregnancies with HCQ exposure in 74 women were assessed. The mean age of the women was 34.2 years, and the median number of previous miscarriages was 5. Concomitant exposure was reported in 78 (78%) pregnancies for prednisone, 56 (56%) pregnancies for LDA, and 41 (41%) pregnancies for LMWH. Sixty-two (62%) pregnancies ended within 12 WG, the other 38 (38%) continuing beyond 12 WG. The risk of experiencing an additional early spontaneous miscarriage increased with the number of previous miscarriages, but not with age. The distributions of anomalies identified in RPL investigations and of exposure to other drugs were similar between pregnancies lasting ≤12 WG and those continuing beyond 12WG. The incidence of pregnancies progressing beyond 12 WG was not higher among pregnancies with at least one positive autoantibody (Ab) (i.e. antinuclear Ab titer ≥1:160, ≥1 positive conventional and/or non-conventional antiphospholipid Ab, and/or positive results for ≥1 antithyroid Ab) without diminished ovarian reserve (18/51, 35.3%) than among those without such autoantibody (18/45, 40.0%) (P = 0.63). Multivariate analysis showed that having ≤4 prior miscarriages was the only factor significantly predictive for achieving a pregnancy > 12 WG, after adjustment for age and duration of HCQ use prior to conception (adjusted odds ratio (OR) = 3.13 [1.31-7.83], P = 0.01).</p><p><strong>Limitations, reasons for caution: </strong>Our study has limitations, including the absence of a control group, incomplete data for the diagnostic procedure for RPL in some patients, and the unavailability of results from endometrial biopsies, as well as information about paternal age and behavioral factors. Consequently, not all potential confounding factors could be considered.</p><p><strong>Wider implications of the findings: </strong>Exposure to HCQ in early pregnancy for women with a history of RPL does not seem to prevent further miscarriages, suggesting limited impact on mechanisms related to the maternal immune system.</p><p><strong>Study funding/competing interest(s): </strong>The research received no specific funding, and the authors declare no competing interests.</p><p><strong>Trial registration number: </strong>clinicaltrial.gov NCT05557201.</p>","PeriodicalId":13003,"journal":{"name":"Human reproduction","volume":" ","pages":"1934-1941"},"PeriodicalIF":6.8000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11373309/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hydroxychloroquine in recurrent pregnancy loss: data from a French prospective multicenter registry.\",\"authors\":\"Amandine Dernoncourt, Kaies Hedhli, Noémie Abisror, Meryam Cheloufi, Jonathan Cohen, Kamila Kolanska, Chloé McAvoy, Lise Selleret, Eric Ballot, Emmanuelle Mathieu d'Argent, Nathalie Chabbert Buffet, Olivier Fain, Gilles Kayem, Arsène Mekinian\",\"doi\":\"10.1093/humrep/deae146\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study question: </strong>What are the outcomes of pregnancies exposed to hydroxychloroquine (HCQ) in women with a history of recurrent pregnancy loss (RPL), and what factors predict the course of these pregnancies beyond the first trimester?</p><p><strong>Summary answer: </strong>In our cohort of pregnancies in women with a history of RPL exposed to HCQ early in pregnancy, we found that the only factor determining the success of these pregnancies was the number of previous miscarriages.</p><p><strong>What is known already: </strong>Dysregulation of the maternal immune system plays a role in RPL. HCQ, with its dual immunomodulating and vascular protective effects, is a potential treatment for unexplained RPL.</p><p><strong>Study design, size, duration: </strong>The FALCO (Facteurs de récidive précoce des fausses couches) registry is an ongoing French multicenter infertility registry established in 2017 that includes women (aged from 18 to 49 years) with a history of spontaneous RPL (at least three early miscarriages (≤12 weeks of gestation (WG)) recruited from several university hospitals.</p><p><strong>Participants/materials, setting, methods: </strong>Spontaneous pregnancies enrolled in the FALCO registry with an exposure to HCQ (before conception or at the start of pregnancy) were included. Pregnancies concomitantly exposed to tumor necrosis factor inhibitors, interleukin-1 and -2 inhibitors, intravenous immunoglobulin, and/or intravenous intralipid infusion, were excluded. Concomitant treatment with low-dose aspirin (LDA), low-molecular weight heparin (LMWH), progesterone, and/or prednisone was allowed. All patients underwent the recommended evaluations for investigating RPL. Those who became pregnant received obstetric care in accordance with French recommendations and were followed prospectively. The main endpoint was the occurrence of a pregnancy continuing beyond 12 WG, and the secondary endpoint was the occurrence of a live birth.</p><p><strong>Main results and the role of chance: </strong>One hundred pregnancies with HCQ exposure in 74 women were assessed. The mean age of the women was 34.2 years, and the median number of previous miscarriages was 5. Concomitant exposure was reported in 78 (78%) pregnancies for prednisone, 56 (56%) pregnancies for LDA, and 41 (41%) pregnancies for LMWH. Sixty-two (62%) pregnancies ended within 12 WG, the other 38 (38%) continuing beyond 12 WG. The risk of experiencing an additional early spontaneous miscarriage increased with the number of previous miscarriages, but not with age. The distributions of anomalies identified in RPL investigations and of exposure to other drugs were similar between pregnancies lasting ≤12 WG and those continuing beyond 12WG. The incidence of pregnancies progressing beyond 12 WG was not higher among pregnancies with at least one positive autoantibody (Ab) (i.e. antinuclear Ab titer ≥1:160, ≥1 positive conventional and/or non-conventional antiphospholipid Ab, and/or positive results for ≥1 antithyroid Ab) without diminished ovarian reserve (18/51, 35.3%) than among those without such autoantibody (18/45, 40.0%) (P = 0.63). Multivariate analysis showed that having ≤4 prior miscarriages was the only factor significantly predictive for achieving a pregnancy > 12 WG, after adjustment for age and duration of HCQ use prior to conception (adjusted odds ratio (OR) = 3.13 [1.31-7.83], P = 0.01).</p><p><strong>Limitations, reasons for caution: </strong>Our study has limitations, including the absence of a control group, incomplete data for the diagnostic procedure for RPL in some patients, and the unavailability of results from endometrial biopsies, as well as information about paternal age and behavioral factors. Consequently, not all potential confounding factors could be considered.</p><p><strong>Wider implications of the findings: </strong>Exposure to HCQ in early pregnancy for women with a history of RPL does not seem to prevent further miscarriages, suggesting limited impact on mechanisms related to the maternal immune system.</p><p><strong>Study funding/competing interest(s): </strong>The research received no specific funding, and the authors declare no competing interests.</p><p><strong>Trial registration number: </strong>clinicaltrial.gov NCT05557201.</p>\",\"PeriodicalId\":13003,\"journal\":{\"name\":\"Human reproduction\",\"volume\":\" \",\"pages\":\"1934-1941\"},\"PeriodicalIF\":6.8000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11373309/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human reproduction\",\"FirstCategoryId\":\"88\",\"ListUrlMain\":\"https://doi.org/10.1093/humrep/deae146\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction","FirstCategoryId":"88","ListUrlMain":"https://doi.org/10.1093/humrep/deae146","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Hydroxychloroquine in recurrent pregnancy loss: data from a French prospective multicenter registry.
Study question: What are the outcomes of pregnancies exposed to hydroxychloroquine (HCQ) in women with a history of recurrent pregnancy loss (RPL), and what factors predict the course of these pregnancies beyond the first trimester?
Summary answer: In our cohort of pregnancies in women with a history of RPL exposed to HCQ early in pregnancy, we found that the only factor determining the success of these pregnancies was the number of previous miscarriages.
What is known already: Dysregulation of the maternal immune system plays a role in RPL. HCQ, with its dual immunomodulating and vascular protective effects, is a potential treatment for unexplained RPL.
Study design, size, duration: The FALCO (Facteurs de récidive précoce des fausses couches) registry is an ongoing French multicenter infertility registry established in 2017 that includes women (aged from 18 to 49 years) with a history of spontaneous RPL (at least three early miscarriages (≤12 weeks of gestation (WG)) recruited from several university hospitals.
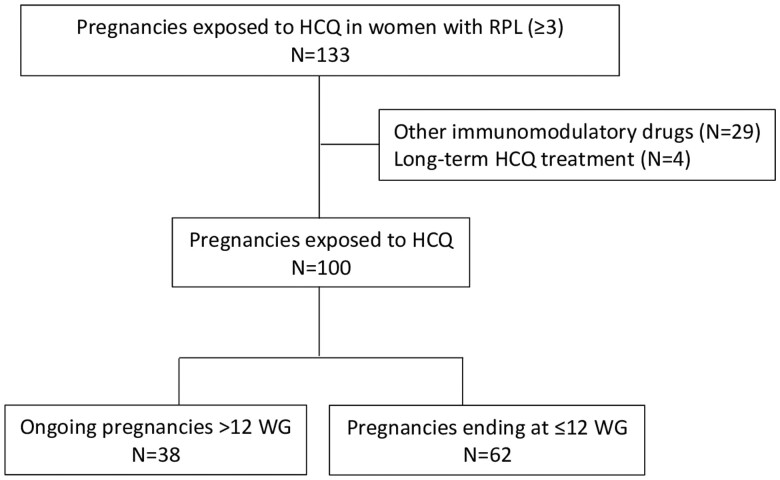
Participants/materials, setting, methods: Spontaneous pregnancies enrolled in the FALCO registry with an exposure to HCQ (before conception or at the start of pregnancy) were included. Pregnancies concomitantly exposed to tumor necrosis factor inhibitors, interleukin-1 and -2 inhibitors, intravenous immunoglobulin, and/or intravenous intralipid infusion, were excluded. Concomitant treatment with low-dose aspirin (LDA), low-molecular weight heparin (LMWH), progesterone, and/or prednisone was allowed. All patients underwent the recommended evaluations for investigating RPL. Those who became pregnant received obstetric care in accordance with French recommendations and were followed prospectively. The main endpoint was the occurrence of a pregnancy continuing beyond 12 WG, and the secondary endpoint was the occurrence of a live birth.
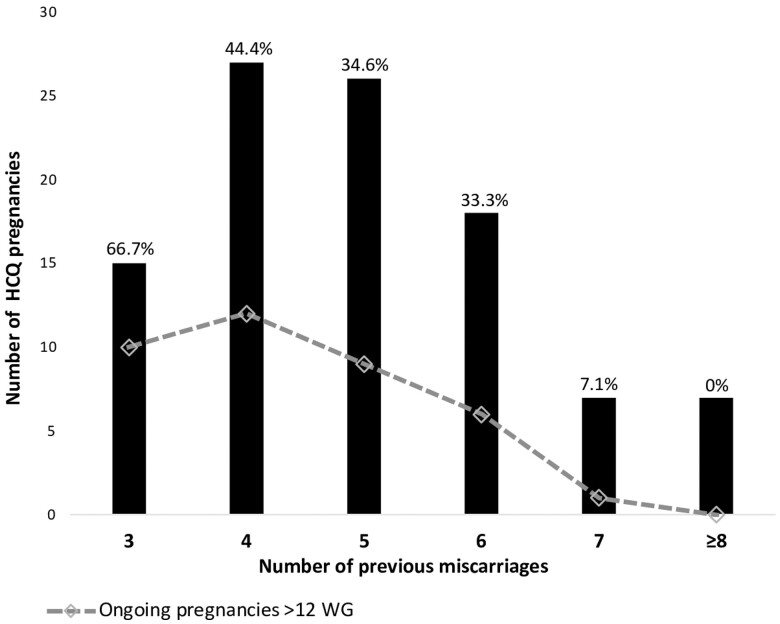
Main results and the role of chance: One hundred pregnancies with HCQ exposure in 74 women were assessed. The mean age of the women was 34.2 years, and the median number of previous miscarriages was 5. Concomitant exposure was reported in 78 (78%) pregnancies for prednisone, 56 (56%) pregnancies for LDA, and 41 (41%) pregnancies for LMWH. Sixty-two (62%) pregnancies ended within 12 WG, the other 38 (38%) continuing beyond 12 WG. The risk of experiencing an additional early spontaneous miscarriage increased with the number of previous miscarriages, but not with age. The distributions of anomalies identified in RPL investigations and of exposure to other drugs were similar between pregnancies lasting ≤12 WG and those continuing beyond 12WG. The incidence of pregnancies progressing beyond 12 WG was not higher among pregnancies with at least one positive autoantibody (Ab) (i.e. antinuclear Ab titer ≥1:160, ≥1 positive conventional and/or non-conventional antiphospholipid Ab, and/or positive results for ≥1 antithyroid Ab) without diminished ovarian reserve (18/51, 35.3%) than among those without such autoantibody (18/45, 40.0%) (P = 0.63). Multivariate analysis showed that having ≤4 prior miscarriages was the only factor significantly predictive for achieving a pregnancy > 12 WG, after adjustment for age and duration of HCQ use prior to conception (adjusted odds ratio (OR) = 3.13 [1.31-7.83], P = 0.01).
Limitations, reasons for caution: Our study has limitations, including the absence of a control group, incomplete data for the diagnostic procedure for RPL in some patients, and the unavailability of results from endometrial biopsies, as well as information about paternal age and behavioral factors. Consequently, not all potential confounding factors could be considered.
Wider implications of the findings: Exposure to HCQ in early pregnancy for women with a history of RPL does not seem to prevent further miscarriages, suggesting limited impact on mechanisms related to the maternal immune system.
Study funding/competing interest(s): The research received no specific funding, and the authors declare no competing interests.
期刊介绍:
Human Reproduction features full-length, peer-reviewed papers reporting original research, concise clinical case reports, as well as opinions and debates on topical issues.
Papers published cover the clinical science and medical aspects of reproductive physiology, pathology and endocrinology; including andrology, gonad function, gametogenesis, fertilization, embryo development, implantation, early pregnancy, genetics, genetic diagnosis, oncology, infectious disease, surgery, contraception, infertility treatment, psychology, ethics and social issues.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
