Sarah I. Daniels PhD, Shayna Cave MS, Todd H. Wagner PhD, Taryn A. Perez MS, Sara N. Edmond PhD, William C. Becker MD, Amanda M. Midboe PhD
{"title":"退伍军人健康管理局多学科复杂疼痛诊所的实施、干预和下游成本。","authors":"Sarah I. Daniels PhD, Shayna Cave MS, Todd H. Wagner PhD, Taryn A. Perez MS, Sara N. Edmond PhD, William C. Becker MD, Amanda M. Midboe PhD","doi":"10.1111/1475-6773.14345","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>To determine the budget impact of implementing multidisciplinary complex pain clinics (MCPCs) for Veterans Health Administration (VA) patients living with complex chronic pain and substance use disorder comorbidities who are on risky opioid regimens.</p>\n </section>\n \n <section>\n \n <h3> Data Sources and Study Setting</h3>\n \n <p>We measured implementation costs for three MCPCs over 2 years using micro-costing methods. Intervention and downstream costs were obtained from the VA Managerial Cost Accounting System from 2 years prior to 2 years after opening of MCPCs.</p>\n </section>\n \n <section>\n \n <h3> Study Design</h3>\n \n <p>Staff at the three VA sites implementing MCPCs were supported by Implementation Facilitation. The intervention cohort was patients at MCPC sites who received treatment based on their history of chronic pain and risky opioid use. Intervention costs and downstream costs were estimated with a quasi-experimental study design using a propensity score-weighted difference-in-difference approach. The healthcare utilization costs of treated patients were compared with a control group having clinically similar characteristics and undergoing the standard route of care at neighboring VA medical centers. Cancer and hospice patients were excluded.</p>\n </section>\n \n <section>\n \n <h3> Data Collection/Extraction Methods</h3>\n \n <p>Activity-based costing data acquired from MCPC sites were used to estimate implementation costs. Intervention and downstream costs were extracted from VA administrative data.</p>\n </section>\n \n <section>\n \n <h3> Principal Findings</h3>\n \n <p>Average Implementation Facilitation costs ranged from $380 to $640 per month for each site. Upon opening of three MCPCs, average intervention costs per patient were significantly higher than the control group at two intervention sites. Downstream costs were significantly higher at only one of three intervention sites. Site-level differences were due to variation in inpatient costs, with some confounding likely due to the COVID-19 pandemic. This evidence suggests that necessary start-up investments are required to initiate MCPCs, with allocations of funds needed for implementation, intervention, and downstream costs.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Incorporating implementation, intervention, and downstream costs in this evaluation provides a thorough budget impact analysis, which decision-makers may use when considering whether to expand effective programming.</p>\n </section>\n </div>","PeriodicalId":55065,"journal":{"name":"Health Services Research","volume":"59 S2","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2024-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11540574/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementation, intervention, and downstream costs for implementation of a multidisciplinary complex pain clinic in the Veterans Health Administration\",\"authors\":\"Sarah I. Daniels PhD, Shayna Cave MS, Todd H. Wagner PhD, Taryn A. Perez MS, Sara N. Edmond PhD, William C. Becker MD, Amanda M. Midboe PhD\",\"doi\":\"10.1111/1475-6773.14345\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>To determine the budget impact of implementing multidisciplinary complex pain clinics (MCPCs) for Veterans Health Administration (VA) patients living with complex chronic pain and substance use disorder comorbidities who are on risky opioid regimens.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Data Sources and Study Setting</h3>\\n \\n <p>We measured implementation costs for three MCPCs over 2 years using micro-costing methods. Intervention and downstream costs were obtained from the VA Managerial Cost Accounting System from 2 years prior to 2 years after opening of MCPCs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Study Design</h3>\\n \\n <p>Staff at the three VA sites implementing MCPCs were supported by Implementation Facilitation. The intervention cohort was patients at MCPC sites who received treatment based on their history of chronic pain and risky opioid use. Intervention costs and downstream costs were estimated with a quasi-experimental study design using a propensity score-weighted difference-in-difference approach. The healthcare utilization costs of treated patients were compared with a control group having clinically similar characteristics and undergoing the standard route of care at neighboring VA medical centers. Cancer and hospice patients were excluded.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Data Collection/Extraction Methods</h3>\\n \\n <p>Activity-based costing data acquired from MCPC sites were used to estimate implementation costs. Intervention and downstream costs were extracted from VA administrative data.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Principal Findings</h3>\\n \\n <p>Average Implementation Facilitation costs ranged from $380 to $640 per month for each site. Upon opening of three MCPCs, average intervention costs per patient were significantly higher than the control group at two intervention sites. Downstream costs were significantly higher at only one of three intervention sites. Site-level differences were due to variation in inpatient costs, with some confounding likely due to the COVID-19 pandemic. This evidence suggests that necessary start-up investments are required to initiate MCPCs, with allocations of funds needed for implementation, intervention, and downstream costs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Incorporating implementation, intervention, and downstream costs in this evaluation provides a thorough budget impact analysis, which decision-makers may use when considering whether to expand effective programming.</p>\\n </section>\\n </div>\",\"PeriodicalId\":55065,\"journal\":{\"name\":\"Health Services Research\",\"volume\":\"59 S2\",\"pages\":\"\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-07-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11540574/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Services Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/1475-6773.14345\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1475-6773.14345","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Implementation, intervention, and downstream costs for implementation of a multidisciplinary complex pain clinic in the Veterans Health Administration
Objective
To determine the budget impact of implementing multidisciplinary complex pain clinics (MCPCs) for Veterans Health Administration (VA) patients living with complex chronic pain and substance use disorder comorbidities who are on risky opioid regimens.
Data Sources and Study Setting
We measured implementation costs for three MCPCs over 2 years using micro-costing methods. Intervention and downstream costs were obtained from the VA Managerial Cost Accounting System from 2 years prior to 2 years after opening of MCPCs.
Study Design
Staff at the three VA sites implementing MCPCs were supported by Implementation Facilitation. The intervention cohort was patients at MCPC sites who received treatment based on their history of chronic pain and risky opioid use. Intervention costs and downstream costs were estimated with a quasi-experimental study design using a propensity score-weighted difference-in-difference approach. The healthcare utilization costs of treated patients were compared with a control group having clinically similar characteristics and undergoing the standard route of care at neighboring VA medical centers. Cancer and hospice patients were excluded.
Data Collection/Extraction Methods
Activity-based costing data acquired from MCPC sites were used to estimate implementation costs. Intervention and downstream costs were extracted from VA administrative data.
Principal Findings
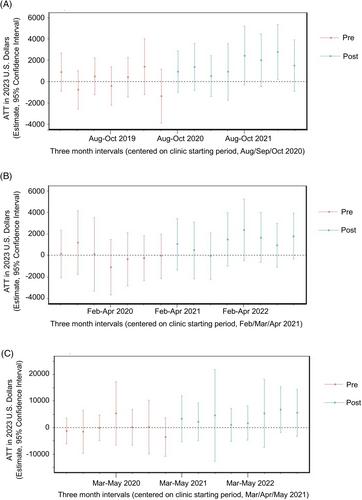
Average Implementation Facilitation costs ranged from $380 to $640 per month for each site. Upon opening of three MCPCs, average intervention costs per patient were significantly higher than the control group at two intervention sites. Downstream costs were significantly higher at only one of three intervention sites. Site-level differences were due to variation in inpatient costs, with some confounding likely due to the COVID-19 pandemic. This evidence suggests that necessary start-up investments are required to initiate MCPCs, with allocations of funds needed for implementation, intervention, and downstream costs.
Conclusions
Incorporating implementation, intervention, and downstream costs in this evaluation provides a thorough budget impact analysis, which decision-makers may use when considering whether to expand effective programming.
期刊介绍:
Health Services Research (HSR) is a peer-reviewed scholarly journal that provides researchers and public and private policymakers with the latest research findings, methods, and concepts related to the financing, organization, delivery, evaluation, and outcomes of health services. Rated as one of the top journals in the fields of health policy and services and health care administration, HSR publishes outstanding articles reporting the findings of original investigations that expand knowledge and understanding of the wide-ranging field of health care and that will help to improve the health of individuals and communities.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
