Shusuke Akamatsu, Yushi Naito, Jun Nagayama, Yuta Sano, Satoshi Inoue, Kazuna Matsuo, Tomoyasu Sano, Shohei Ishida, Yoshihisa Matsukawa, Masashi Kato
{"title":"新发转移性阉割敏感性前列腺癌的治疗升级和降级。","authors":"Shusuke Akamatsu, Yushi Naito, Jun Nagayama, Yuta Sano, Satoshi Inoue, Kazuna Matsuo, Tomoyasu Sano, Shohei Ishida, Yoshihisa Matsukawa, Masashi Kato","doi":"10.18999/nagjms.86.2.169","DOIUrl":null,"url":null,"abstract":"<p><p>Androgen receptor signaling inhibitors combined with androgen deprivation therapy have become the standard of care for metastatic castration-sensitive prostate cancer (mCSPC), regardless of tumor volume or risk. However, survival of approximately one-third of these patients has not improved, necessitating further treatment escalation. On the other hand, for patients with oligometastatic mCSPC, there is an emerging role for local radiation therapy. Although data remain scarce, it is expected that treatment of both primary tumor as well as metastasis-directed therapy may improve survival outcomes. In these patients, systemic therapy may be de-escalated to intermittent therapy. However, precise risk stratification is necessary for risk-based treatment escalation or de-escalation. In addition to risk stratification based on clinical parameters, research has been conducted to incorporate genomic and/or transcriptomic data into risk stratification. In future, an integrated risk model is expected to precisely stratify patients and guide treatment strategies. Here, we first review the transition of the standard treatment for mCSPC over the last decade and further discuss the newest concept of escalating or de-escalating treatment using a multi-modal approach based on the currently available literature.</p>","PeriodicalId":49014,"journal":{"name":"Nagoya Journal of Medical Science","volume":"86 2","pages":"169-180"},"PeriodicalIF":0.9000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11219222/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment escalation and de-escalation of de-novo metastatic castration-sensitive prostate cancer.\",\"authors\":\"Shusuke Akamatsu, Yushi Naito, Jun Nagayama, Yuta Sano, Satoshi Inoue, Kazuna Matsuo, Tomoyasu Sano, Shohei Ishida, Yoshihisa Matsukawa, Masashi Kato\",\"doi\":\"10.18999/nagjms.86.2.169\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Androgen receptor signaling inhibitors combined with androgen deprivation therapy have become the standard of care for metastatic castration-sensitive prostate cancer (mCSPC), regardless of tumor volume or risk. However, survival of approximately one-third of these patients has not improved, necessitating further treatment escalation. On the other hand, for patients with oligometastatic mCSPC, there is an emerging role for local radiation therapy. Although data remain scarce, it is expected that treatment of both primary tumor as well as metastasis-directed therapy may improve survival outcomes. In these patients, systemic therapy may be de-escalated to intermittent therapy. However, precise risk stratification is necessary for risk-based treatment escalation or de-escalation. In addition to risk stratification based on clinical parameters, research has been conducted to incorporate genomic and/or transcriptomic data into risk stratification. In future, an integrated risk model is expected to precisely stratify patients and guide treatment strategies. Here, we first review the transition of the standard treatment for mCSPC over the last decade and further discuss the newest concept of escalating or de-escalating treatment using a multi-modal approach based on the currently available literature.</p>\",\"PeriodicalId\":49014,\"journal\":{\"name\":\"Nagoya Journal of Medical Science\",\"volume\":\"86 2\",\"pages\":\"169-180\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11219222/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nagoya Journal of Medical Science\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.18999/nagjms.86.2.169\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nagoya Journal of Medical Science","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.18999/nagjms.86.2.169","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Treatment escalation and de-escalation of de-novo metastatic castration-sensitive prostate cancer.
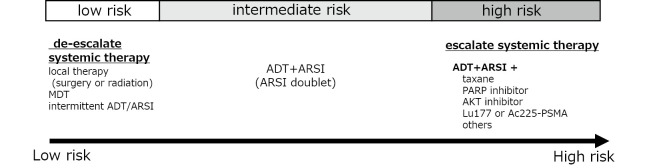
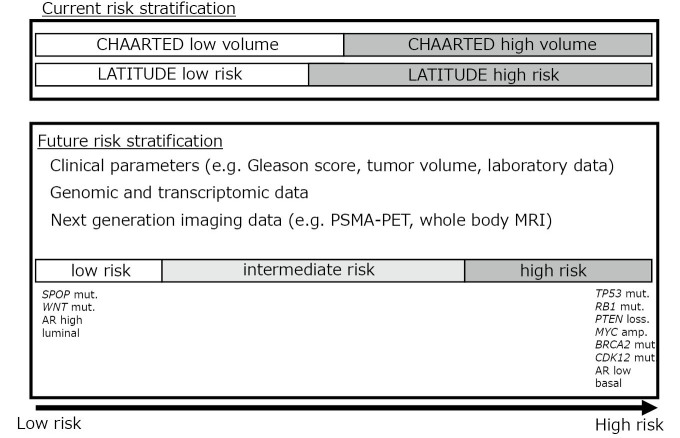
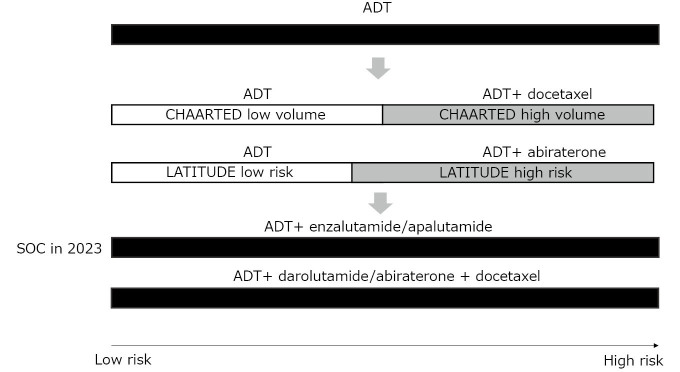
Androgen receptor signaling inhibitors combined with androgen deprivation therapy have become the standard of care for metastatic castration-sensitive prostate cancer (mCSPC), regardless of tumor volume or risk. However, survival of approximately one-third of these patients has not improved, necessitating further treatment escalation. On the other hand, for patients with oligometastatic mCSPC, there is an emerging role for local radiation therapy. Although data remain scarce, it is expected that treatment of both primary tumor as well as metastasis-directed therapy may improve survival outcomes. In these patients, systemic therapy may be de-escalated to intermittent therapy. However, precise risk stratification is necessary for risk-based treatment escalation or de-escalation. In addition to risk stratification based on clinical parameters, research has been conducted to incorporate genomic and/or transcriptomic data into risk stratification. In future, an integrated risk model is expected to precisely stratify patients and guide treatment strategies. Here, we first review the transition of the standard treatment for mCSPC over the last decade and further discuss the newest concept of escalating or de-escalating treatment using a multi-modal approach based on the currently available literature.
期刊介绍:
The Journal publishes original papers in the areas of medical science and its related fields. Reviews, symposium reports, short communications, notes, case reports, hypothesis papers, medical image at a glance, video and announcements are also accepted.
Manuscripts should be in English. It is recommended that an English check of the manuscript by a competent and knowledgeable native speaker be completed before submission.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
