Lorenzo Huang, Fariba Fallahzadeh, Gauti Jóhannesson
{"title":"隐匿性 GCA:巨细胞动脉炎的罕见变种","authors":"Lorenzo Huang, Fariba Fallahzadeh, Gauti Jóhannesson","doi":"10.1111/aos.16731","DOIUrl":null,"url":null,"abstract":"<p>An 82-year-old Scandinavian woman with hypertension and diabetes mellitus type 2 experienced 1–2 seconds of blurred vision alternating between right and left eye, never together. There were no associated symptoms such as fatigue, headache or jaw claudication, no sign of temporary visual field loss or ‘dark curtain’. The visual acuity was 0.6/0.6 Snellen explained by moderate cataract with pseudo exfoliation, normal bilateral intraocular pressure and fundoscopy that revealed optic disks with normal size and features bilaterally. There was bilateral calcification-like deposit on the central cornea, initially thought to explain her brief visual disturbances. She was discharged with tear substitutes and instructed to return in case of worsening of symptoms.</p><p>The patient contacted the clinic a week later, reporting altitudinal lower visual field loss in her left eye that worsened to almost total visual loss (Figure 1a). Upon examination, the patient confirmed again absence of the above-mentioned symptoms (no temporal/generalized headache, jaw claudication, scalp pain while combing hair or polymyalgia rheumatica symptoms), no signs of confusion, tiredness, neurological abnormalities, pain in the eye, weight loss or fever. She was a non-smoker and did not have sleep apnoea. Her left eye had 0.4 Snellen visual acuity, optic disc swelling (Figure 1b), no signs of retinal ischemia and a positive left relative afferent pupillary defect (RAPD). C-reactive protein (CRP) and sedimentation rate (SR) were normal, orbital magnetic resonance imaging (MRI) showed no optic abnormalities that could explain the visual field loss. Despite the lack of giant cell arteritis (GCA) symptoms, a rheumatologist was consulted and according to his assessment, an ultrasound (US) evaluation was not deemed necessary. The patient was diagnosed with left sided non-arteritic anterior ischemic optic neuropathy (NA-AION) with a referral to the general practitioner for further cardiovascular risk evaluation.</p><p>The patient was followed up with periodical visual field and visual acuity assessment without reporting new vision deterioration. An additional neck-brain angiography showed no significant findings such as endangering stenosis and the patient was treated with 40 mg oral prednisolone for 2 weeks. Over 2 months of follow up, the left visual field improved from visual field index (VFI) 8–24% and the left optic disc swelling regressed to optic atrophy.</p><p>The patient contacted the eye clinic 3 weeks before the planned final-check due to sudden upper altitudinal hemianopia in her right eye and worsening of her remaining left visual field (Figure 2a). Like before, the patient was totally asymptomatic, no symptoms as listed above besides the sudden right visual field loss. The examinations revealed worsening of visual acuity (0.4/0.3), a fresh right optic disc swelling (Figure 2b) and optic disc atrophy on the left (Figure 2c). Due to bilateral worsening with neither GCA symptoms nor inflammatory markers elevation, the patient was referred to the emergency department for suspected stroke or new onset of Space Occupying Lesion (SOL) and bilateral NA-AION as differential diagnosis.</p><p>After a normal computer tomography without new vascular pathologies the emergency doctor, in consultation with a neurologist, initiated a temporary double anticoagulant therapy and the patient was booked for a new evaluation at the neurology department.</p><p>Although the likelihood of Arteritic AION (A-AION) was deemed highly unlikely, a new rheumatology consultation for a temporal artery ultrasound assessment was suggested. The sonography showed a characteristic halo-sign in multiple branches of the temporal artery bilaterally (Figure 3a–c) and occasionally thickened wall on the distal part of the left axillary artery (Figure 3d), leading to the diagnosis of GCA. However, the patient did not want to perform a Temporal Artery Biopsy (TAB) due to anxiety and according to the local guidelines, a positive US halo-sign is sufficient to confirm an active GCA. Intravenous methylprednisolone was initiated followed by slow tapered oral prednisolone.</p><p>The patient visual status did not deteriorate following aggressive corticosteroid treatment according to her latest visual field test (Figure 4).</p><p>Giant Cell Arteritis (GCA) is a chronic granulomatous inflammation of medium-to-large arteries that affects commonly the carotid artery and its branches causing classical symptoms such as fever, temporal tenderness, jaw claudication, polymyalgia rheumatica (PMR) complaints and, if untreated, visual field loss (Zaragoza et al., <span>2015</span>).</p><p>According to a previous meta-analysis, the incidence of GCA is 10 cases per 100 000 people above the 50 years of age, highest in Scandinavia 21.6 [18.9, 24.2], followed by North and South America 10.9, Europe 7.3 and Oceania 7.9 (Li et al., <span>2021</span>).</p><p>Focal GCA symptoms develop because the vascular inflammation involves areas that are supplied by affected peripheral vessels (therefore temporal headache, jaw claudication and rare cases of tongue necrosis). However, the GCA picture is very variable, and therefore, the patients do not always present with all these classic symptoms.</p><p>Based on this clinical case development and findings, the above-mentioned patient was diagnosed with Occult GCA, an ocular variant of GCA with an incidence of 14.3% (Issa et al., <span>2022</span>) and up to 21.2% characterized by an absence of systemic symptoms and signs commonly associated with GCA (Hayreh et al., <span>1998</span>). The patient showed neither elevation of inflammatory markers nor systemic symptoms besides AION and visual field defects bilaterally, a very rare exception.</p><p>Bilateral NA-AION could be a possible differential diagnosis but the diagnosis of A-AION is supported by the ultrasound examination which was conducted by two distinct professionals. The examination revealed halo-signs across multiple arterial branches bilaterally. The halo-signs were seen on both the right and left a. temporalis with occasional presence of thickened wall of the left distal a. axillaris. Atherosclerosis was ruled out and thus, these findings confirmed the suspicion of GCA. Furthermore, the cessation of bilateral visual field deterioration coincided with the commencement of aggressive corticosteroid therapy, which is a therapy that yields no significant benefits in NA-AION (Hayreh & Zimmerman, <span>2008</span>).</p><p>Since Northern European regions have a higher risk for GCA development, it is reasonable that Scandinavian physicians should be familiarized with this rare GCA variant, maintain a low threshold for GCA testing in the relevant demographic group and leveraging cost-effective ultrasound examinations can be beneficial in early detection and management.</p><p>In case of bilateral sequential AION in patients above the age of 50 it is advised to implement temporal artery sonographic examination to exclude the possibility of an Occult GCA. However, it is crucial to differentiate the US halo-sign between the arterial intimal thickening (characteristic of GCA) and atherosclerosis.</p><p>According to the 2023 EULAR recommendation, US of temporal and axillary arteries should be considered as the first-line imaging modality to investigate suspected GCA (Dejaco et al., <span>2023</span>). In cases of sequential bilateral AION, if uncertainty remains despite ultrasound evaluation, other diagnostic imaging are suggested and further differential diagnosis should be considered such as optic neuritis, SOL, Foster-Kennedy Syndrome (FSK) by a skull base tumour and pseudo-FSK, IIH, sarcoidosis and hypertensive crisis. Temporal Artery Biopsy (TAB) is the gold standard for GCA diagnosis; however, it is invasive with inherent risks as well as unreliable due to tissue sampling (Crain et al., <span>2021</span>).</p><p>This case highlights also ultrasound's pivotal role in modern GCA detection, enhancing diagnostic accuracy in a disease that shows a very diverse clinical presentation. This cost-effective and quick investigation can be vision saving in asymptomatic patients or geriatric populations that are too old to show specific GCA symptoms, group-at-risk that is ever-increasing in the modern western society.</p>","PeriodicalId":6915,"journal":{"name":"Acta Ophthalmologica","volume":"102 8","pages":"968-973"},"PeriodicalIF":2.8000,"publicationDate":"2024-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aos.16731","citationCount":"0","resultStr":"{\"title\":\"Occult GCA: A rare variant of Giant Cell Arteritis\",\"authors\":\"Lorenzo Huang, Fariba Fallahzadeh, Gauti Jóhannesson\",\"doi\":\"10.1111/aos.16731\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>An 82-year-old Scandinavian woman with hypertension and diabetes mellitus type 2 experienced 1–2 seconds of blurred vision alternating between right and left eye, never together. There were no associated symptoms such as fatigue, headache or jaw claudication, no sign of temporary visual field loss or ‘dark curtain’. The visual acuity was 0.6/0.6 Snellen explained by moderate cataract with pseudo exfoliation, normal bilateral intraocular pressure and fundoscopy that revealed optic disks with normal size and features bilaterally. There was bilateral calcification-like deposit on the central cornea, initially thought to explain her brief visual disturbances. She was discharged with tear substitutes and instructed to return in case of worsening of symptoms.</p><p>The patient contacted the clinic a week later, reporting altitudinal lower visual field loss in her left eye that worsened to almost total visual loss (Figure 1a). Upon examination, the patient confirmed again absence of the above-mentioned symptoms (no temporal/generalized headache, jaw claudication, scalp pain while combing hair or polymyalgia rheumatica symptoms), no signs of confusion, tiredness, neurological abnormalities, pain in the eye, weight loss or fever. She was a non-smoker and did not have sleep apnoea. Her left eye had 0.4 Snellen visual acuity, optic disc swelling (Figure 1b), no signs of retinal ischemia and a positive left relative afferent pupillary defect (RAPD). C-reactive protein (CRP) and sedimentation rate (SR) were normal, orbital magnetic resonance imaging (MRI) showed no optic abnormalities that could explain the visual field loss. Despite the lack of giant cell arteritis (GCA) symptoms, a rheumatologist was consulted and according to his assessment, an ultrasound (US) evaluation was not deemed necessary. The patient was diagnosed with left sided non-arteritic anterior ischemic optic neuropathy (NA-AION) with a referral to the general practitioner for further cardiovascular risk evaluation.</p><p>The patient was followed up with periodical visual field and visual acuity assessment without reporting new vision deterioration. An additional neck-brain angiography showed no significant findings such as endangering stenosis and the patient was treated with 40 mg oral prednisolone for 2 weeks. Over 2 months of follow up, the left visual field improved from visual field index (VFI) 8–24% and the left optic disc swelling regressed to optic atrophy.</p><p>The patient contacted the eye clinic 3 weeks before the planned final-check due to sudden upper altitudinal hemianopia in her right eye and worsening of her remaining left visual field (Figure 2a). Like before, the patient was totally asymptomatic, no symptoms as listed above besides the sudden right visual field loss. The examinations revealed worsening of visual acuity (0.4/0.3), a fresh right optic disc swelling (Figure 2b) and optic disc atrophy on the left (Figure 2c). Due to bilateral worsening with neither GCA symptoms nor inflammatory markers elevation, the patient was referred to the emergency department for suspected stroke or new onset of Space Occupying Lesion (SOL) and bilateral NA-AION as differential diagnosis.</p><p>After a normal computer tomography without new vascular pathologies the emergency doctor, in consultation with a neurologist, initiated a temporary double anticoagulant therapy and the patient was booked for a new evaluation at the neurology department.</p><p>Although the likelihood of Arteritic AION (A-AION) was deemed highly unlikely, a new rheumatology consultation for a temporal artery ultrasound assessment was suggested. The sonography showed a characteristic halo-sign in multiple branches of the temporal artery bilaterally (Figure 3a–c) and occasionally thickened wall on the distal part of the left axillary artery (Figure 3d), leading to the diagnosis of GCA. However, the patient did not want to perform a Temporal Artery Biopsy (TAB) due to anxiety and according to the local guidelines, a positive US halo-sign is sufficient to confirm an active GCA. Intravenous methylprednisolone was initiated followed by slow tapered oral prednisolone.</p><p>The patient visual status did not deteriorate following aggressive corticosteroid treatment according to her latest visual field test (Figure 4).</p><p>Giant Cell Arteritis (GCA) is a chronic granulomatous inflammation of medium-to-large arteries that affects commonly the carotid artery and its branches causing classical symptoms such as fever, temporal tenderness, jaw claudication, polymyalgia rheumatica (PMR) complaints and, if untreated, visual field loss (Zaragoza et al., <span>2015</span>).</p><p>According to a previous meta-analysis, the incidence of GCA is 10 cases per 100 000 people above the 50 years of age, highest in Scandinavia 21.6 [18.9, 24.2], followed by North and South America 10.9, Europe 7.3 and Oceania 7.9 (Li et al., <span>2021</span>).</p><p>Focal GCA symptoms develop because the vascular inflammation involves areas that are supplied by affected peripheral vessels (therefore temporal headache, jaw claudication and rare cases of tongue necrosis). However, the GCA picture is very variable, and therefore, the patients do not always present with all these classic symptoms.</p><p>Based on this clinical case development and findings, the above-mentioned patient was diagnosed with Occult GCA, an ocular variant of GCA with an incidence of 14.3% (Issa et al., <span>2022</span>) and up to 21.2% characterized by an absence of systemic symptoms and signs commonly associated with GCA (Hayreh et al., <span>1998</span>). The patient showed neither elevation of inflammatory markers nor systemic symptoms besides AION and visual field defects bilaterally, a very rare exception.</p><p>Bilateral NA-AION could be a possible differential diagnosis but the diagnosis of A-AION is supported by the ultrasound examination which was conducted by two distinct professionals. The examination revealed halo-signs across multiple arterial branches bilaterally. The halo-signs were seen on both the right and left a. temporalis with occasional presence of thickened wall of the left distal a. axillaris. Atherosclerosis was ruled out and thus, these findings confirmed the suspicion of GCA. Furthermore, the cessation of bilateral visual field deterioration coincided with the commencement of aggressive corticosteroid therapy, which is a therapy that yields no significant benefits in NA-AION (Hayreh & Zimmerman, <span>2008</span>).</p><p>Since Northern European regions have a higher risk for GCA development, it is reasonable that Scandinavian physicians should be familiarized with this rare GCA variant, maintain a low threshold for GCA testing in the relevant demographic group and leveraging cost-effective ultrasound examinations can be beneficial in early detection and management.</p><p>In case of bilateral sequential AION in patients above the age of 50 it is advised to implement temporal artery sonographic examination to exclude the possibility of an Occult GCA. However, it is crucial to differentiate the US halo-sign between the arterial intimal thickening (characteristic of GCA) and atherosclerosis.</p><p>According to the 2023 EULAR recommendation, US of temporal and axillary arteries should be considered as the first-line imaging modality to investigate suspected GCA (Dejaco et al., <span>2023</span>). In cases of sequential bilateral AION, if uncertainty remains despite ultrasound evaluation, other diagnostic imaging are suggested and further differential diagnosis should be considered such as optic neuritis, SOL, Foster-Kennedy Syndrome (FSK) by a skull base tumour and pseudo-FSK, IIH, sarcoidosis and hypertensive crisis. Temporal Artery Biopsy (TAB) is the gold standard for GCA diagnosis; however, it is invasive with inherent risks as well as unreliable due to tissue sampling (Crain et al., <span>2021</span>).</p><p>This case highlights also ultrasound's pivotal role in modern GCA detection, enhancing diagnostic accuracy in a disease that shows a very diverse clinical presentation. This cost-effective and quick investigation can be vision saving in asymptomatic patients or geriatric populations that are too old to show specific GCA symptoms, group-at-risk that is ever-increasing in the modern western society.</p>\",\"PeriodicalId\":6915,\"journal\":{\"name\":\"Acta Ophthalmologica\",\"volume\":\"102 8\",\"pages\":\"968-973\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-06-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aos.16731\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Ophthalmologica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/aos.16731\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OPHTHALMOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Ophthalmologica","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/aos.16731","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
Occult GCA: A rare variant of Giant Cell Arteritis
An 82-year-old Scandinavian woman with hypertension and diabetes mellitus type 2 experienced 1–2 seconds of blurred vision alternating between right and left eye, never together. There were no associated symptoms such as fatigue, headache or jaw claudication, no sign of temporary visual field loss or ‘dark curtain’. The visual acuity was 0.6/0.6 Snellen explained by moderate cataract with pseudo exfoliation, normal bilateral intraocular pressure and fundoscopy that revealed optic disks with normal size and features bilaterally. There was bilateral calcification-like deposit on the central cornea, initially thought to explain her brief visual disturbances. She was discharged with tear substitutes and instructed to return in case of worsening of symptoms.
The patient contacted the clinic a week later, reporting altitudinal lower visual field loss in her left eye that worsened to almost total visual loss (Figure 1a). Upon examination, the patient confirmed again absence of the above-mentioned symptoms (no temporal/generalized headache, jaw claudication, scalp pain while combing hair or polymyalgia rheumatica symptoms), no signs of confusion, tiredness, neurological abnormalities, pain in the eye, weight loss or fever. She was a non-smoker and did not have sleep apnoea. Her left eye had 0.4 Snellen visual acuity, optic disc swelling (Figure 1b), no signs of retinal ischemia and a positive left relative afferent pupillary defect (RAPD). C-reactive protein (CRP) and sedimentation rate (SR) were normal, orbital magnetic resonance imaging (MRI) showed no optic abnormalities that could explain the visual field loss. Despite the lack of giant cell arteritis (GCA) symptoms, a rheumatologist was consulted and according to his assessment, an ultrasound (US) evaluation was not deemed necessary. The patient was diagnosed with left sided non-arteritic anterior ischemic optic neuropathy (NA-AION) with a referral to the general practitioner for further cardiovascular risk evaluation.
The patient was followed up with periodical visual field and visual acuity assessment without reporting new vision deterioration. An additional neck-brain angiography showed no significant findings such as endangering stenosis and the patient was treated with 40 mg oral prednisolone for 2 weeks. Over 2 months of follow up, the left visual field improved from visual field index (VFI) 8–24% and the left optic disc swelling regressed to optic atrophy.
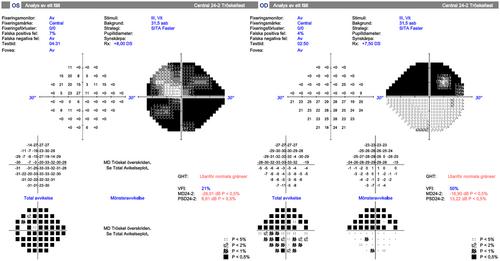
The patient contacted the eye clinic 3 weeks before the planned final-check due to sudden upper altitudinal hemianopia in her right eye and worsening of her remaining left visual field (Figure 2a). Like before, the patient was totally asymptomatic, no symptoms as listed above besides the sudden right visual field loss. The examinations revealed worsening of visual acuity (0.4/0.3), a fresh right optic disc swelling (Figure 2b) and optic disc atrophy on the left (Figure 2c). Due to bilateral worsening with neither GCA symptoms nor inflammatory markers elevation, the patient was referred to the emergency department for suspected stroke or new onset of Space Occupying Lesion (SOL) and bilateral NA-AION as differential diagnosis.
After a normal computer tomography without new vascular pathologies the emergency doctor, in consultation with a neurologist, initiated a temporary double anticoagulant therapy and the patient was booked for a new evaluation at the neurology department.
Although the likelihood of Arteritic AION (A-AION) was deemed highly unlikely, a new rheumatology consultation for a temporal artery ultrasound assessment was suggested. The sonography showed a characteristic halo-sign in multiple branches of the temporal artery bilaterally (Figure 3a–c) and occasionally thickened wall on the distal part of the left axillary artery (Figure 3d), leading to the diagnosis of GCA. However, the patient did not want to perform a Temporal Artery Biopsy (TAB) due to anxiety and according to the local guidelines, a positive US halo-sign is sufficient to confirm an active GCA. Intravenous methylprednisolone was initiated followed by slow tapered oral prednisolone.
The patient visual status did not deteriorate following aggressive corticosteroid treatment according to her latest visual field test (Figure 4).
Giant Cell Arteritis (GCA) is a chronic granulomatous inflammation of medium-to-large arteries that affects commonly the carotid artery and its branches causing classical symptoms such as fever, temporal tenderness, jaw claudication, polymyalgia rheumatica (PMR) complaints and, if untreated, visual field loss (Zaragoza et al., 2015).
According to a previous meta-analysis, the incidence of GCA is 10 cases per 100 000 people above the 50 years of age, highest in Scandinavia 21.6 [18.9, 24.2], followed by North and South America 10.9, Europe 7.3 and Oceania 7.9 (Li et al., 2021).
Focal GCA symptoms develop because the vascular inflammation involves areas that are supplied by affected peripheral vessels (therefore temporal headache, jaw claudication and rare cases of tongue necrosis). However, the GCA picture is very variable, and therefore, the patients do not always present with all these classic symptoms.
Based on this clinical case development and findings, the above-mentioned patient was diagnosed with Occult GCA, an ocular variant of GCA with an incidence of 14.3% (Issa et al., 2022) and up to 21.2% characterized by an absence of systemic symptoms and signs commonly associated with GCA (Hayreh et al., 1998). The patient showed neither elevation of inflammatory markers nor systemic symptoms besides AION and visual field defects bilaterally, a very rare exception.
Bilateral NA-AION could be a possible differential diagnosis but the diagnosis of A-AION is supported by the ultrasound examination which was conducted by two distinct professionals. The examination revealed halo-signs across multiple arterial branches bilaterally. The halo-signs were seen on both the right and left a. temporalis with occasional presence of thickened wall of the left distal a. axillaris. Atherosclerosis was ruled out and thus, these findings confirmed the suspicion of GCA. Furthermore, the cessation of bilateral visual field deterioration coincided with the commencement of aggressive corticosteroid therapy, which is a therapy that yields no significant benefits in NA-AION (Hayreh & Zimmerman, 2008).
Since Northern European regions have a higher risk for GCA development, it is reasonable that Scandinavian physicians should be familiarized with this rare GCA variant, maintain a low threshold for GCA testing in the relevant demographic group and leveraging cost-effective ultrasound examinations can be beneficial in early detection and management.
In case of bilateral sequential AION in patients above the age of 50 it is advised to implement temporal artery sonographic examination to exclude the possibility of an Occult GCA. However, it is crucial to differentiate the US halo-sign between the arterial intimal thickening (characteristic of GCA) and atherosclerosis.
According to the 2023 EULAR recommendation, US of temporal and axillary arteries should be considered as the first-line imaging modality to investigate suspected GCA (Dejaco et al., 2023). In cases of sequential bilateral AION, if uncertainty remains despite ultrasound evaluation, other diagnostic imaging are suggested and further differential diagnosis should be considered such as optic neuritis, SOL, Foster-Kennedy Syndrome (FSK) by a skull base tumour and pseudo-FSK, IIH, sarcoidosis and hypertensive crisis. Temporal Artery Biopsy (TAB) is the gold standard for GCA diagnosis; however, it is invasive with inherent risks as well as unreliable due to tissue sampling (Crain et al., 2021).
This case highlights also ultrasound's pivotal role in modern GCA detection, enhancing diagnostic accuracy in a disease that shows a very diverse clinical presentation. This cost-effective and quick investigation can be vision saving in asymptomatic patients or geriatric populations that are too old to show specific GCA symptoms, group-at-risk that is ever-increasing in the modern western society.
期刊介绍:
Acta Ophthalmologica is published on behalf of the Acta Ophthalmologica Scandinavica Foundation and is the official scientific publication of the following societies: The Danish Ophthalmological Society, The Finnish Ophthalmological Society, The Icelandic Ophthalmological Society, The Norwegian Ophthalmological Society and The Swedish Ophthalmological Society, and also the European Association for Vision and Eye Research (EVER).
Acta Ophthalmologica publishes clinical and experimental original articles, reviews, editorials, educational photo essays (Diagnosis and Therapy in Ophthalmology), case reports and case series, letters to the editor and doctoral theses.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
