Christian Karime, Asrita Vattikonda, Jana G Hashash, Barry G Rosser, Amit Merchea, Luca Stocchi, Francis A Farraye
{"title":"为需要手术干预的炎症性肠病和肝硬化患者成功实施术前经颈静脉肝内门体分流术进行门脉减压。","authors":"Christian Karime, Asrita Vattikonda, Jana G Hashash, Barry G Rosser, Amit Merchea, Luca Stocchi, Francis A Farraye","doi":"10.1093/crocol/otae037","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Colorectal surgery in patients with inflammatory bowel disease (IBD) and cirrhosis has increased morbidity, which may preclude surgery. Preoperative transjugular intrahepatic portosystemic shunt (TIPS) is postulated to reduce surgical risk. In this retrospective single-center study, we characterized perioperative outcomes in patients with IBD and cirrhosis who underwent preoperative TIPS.</p><p><strong>Methods: </strong>We identified patients with IBD and cirrhosis who had undergone preoperative TIPS for portal decompression between 2010 and 2023. All other indications for TIPS led to patient exclusion. Demographic and medical data were collected, including portal pressure measurements. Primary outcome of interest was perioperative outcomes.</p><p><strong>Results: </strong>Ten patients met the inclusion criteria. The most common surgical indications were dysplasia (50%) and refractory IBD (50%). TIPS was performed at a median of 47 days (IQR 34-80) before surgery, with reduction in portal pressures (22.5 vs. 18.5 mmHg, <i>P</i> < .01) and portosystemic gradient (12.5 vs. 5.5 mmHg, <i>P</i> < .01). Perioperative complications occurred in 80% of patients, including surgical site bleeding (30%), wound dehiscence (10%), systemic infection (30%), liver function elevation (50%), and coagulopathy (50%). No patients required re-operation, with median length of stay being 7 days (IQR 5.5-9.3). The 30-day readmission rate was 40%, most commonly for infection (75%), with 2 patients having intra-abdominal abscesses and 1 patient with concern for bowel ischemia. Ninety-day and one-year survival was 100% and 90%, respectively. Patients with primary sclerosing cholangitis (PSC)-cirrhosis were noted to have higher perioperative morbidity and a 30-day readmission rate.</p><p><strong>Conclusions: </strong>In patients with IBD and cirrhosis, preoperative TIPS facilitated successful surgical intervention despite heightened risk. Nevertheless, significant complications were noted, in particular for patients with PSC-cirrhosis.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"6 3","pages":"otae037"},"PeriodicalIF":1.8000,"publicationDate":"2024-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11221072/pdf/","citationCount":"0","resultStr":"{\"title\":\"Successful Preoperative Transjugular Intrahepatic Portosystemic Shunt for Portal Decompression in Patients With Inflammatory Bowel Disease and Cirrhosis Requiring Surgical Intervention.\",\"authors\":\"Christian Karime, Asrita Vattikonda, Jana G Hashash, Barry G Rosser, Amit Merchea, Luca Stocchi, Francis A Farraye\",\"doi\":\"10.1093/crocol/otae037\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Colorectal surgery in patients with inflammatory bowel disease (IBD) and cirrhosis has increased morbidity, which may preclude surgery. Preoperative transjugular intrahepatic portosystemic shunt (TIPS) is postulated to reduce surgical risk. In this retrospective single-center study, we characterized perioperative outcomes in patients with IBD and cirrhosis who underwent preoperative TIPS.</p><p><strong>Methods: </strong>We identified patients with IBD and cirrhosis who had undergone preoperative TIPS for portal decompression between 2010 and 2023. All other indications for TIPS led to patient exclusion. Demographic and medical data were collected, including portal pressure measurements. Primary outcome of interest was perioperative outcomes.</p><p><strong>Results: </strong>Ten patients met the inclusion criteria. The most common surgical indications were dysplasia (50%) and refractory IBD (50%). TIPS was performed at a median of 47 days (IQR 34-80) before surgery, with reduction in portal pressures (22.5 vs. 18.5 mmHg, <i>P</i> < .01) and portosystemic gradient (12.5 vs. 5.5 mmHg, <i>P</i> < .01). Perioperative complications occurred in 80% of patients, including surgical site bleeding (30%), wound dehiscence (10%), systemic infection (30%), liver function elevation (50%), and coagulopathy (50%). No patients required re-operation, with median length of stay being 7 days (IQR 5.5-9.3). The 30-day readmission rate was 40%, most commonly for infection (75%), with 2 patients having intra-abdominal abscesses and 1 patient with concern for bowel ischemia. Ninety-day and one-year survival was 100% and 90%, respectively. Patients with primary sclerosing cholangitis (PSC)-cirrhosis were noted to have higher perioperative morbidity and a 30-day readmission rate.</p><p><strong>Conclusions: </strong>In patients with IBD and cirrhosis, preoperative TIPS facilitated successful surgical intervention despite heightened risk. Nevertheless, significant complications were noted, in particular for patients with PSC-cirrhosis.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":\"6 3\",\"pages\":\"otae037\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11221072/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otae037\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otae037","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Successful Preoperative Transjugular Intrahepatic Portosystemic Shunt for Portal Decompression in Patients With Inflammatory Bowel Disease and Cirrhosis Requiring Surgical Intervention.
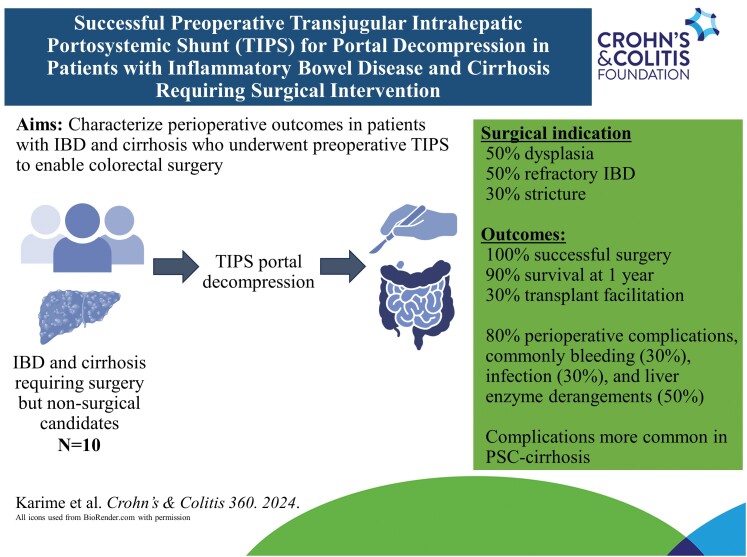
Background: Colorectal surgery in patients with inflammatory bowel disease (IBD) and cirrhosis has increased morbidity, which may preclude surgery. Preoperative transjugular intrahepatic portosystemic shunt (TIPS) is postulated to reduce surgical risk. In this retrospective single-center study, we characterized perioperative outcomes in patients with IBD and cirrhosis who underwent preoperative TIPS.
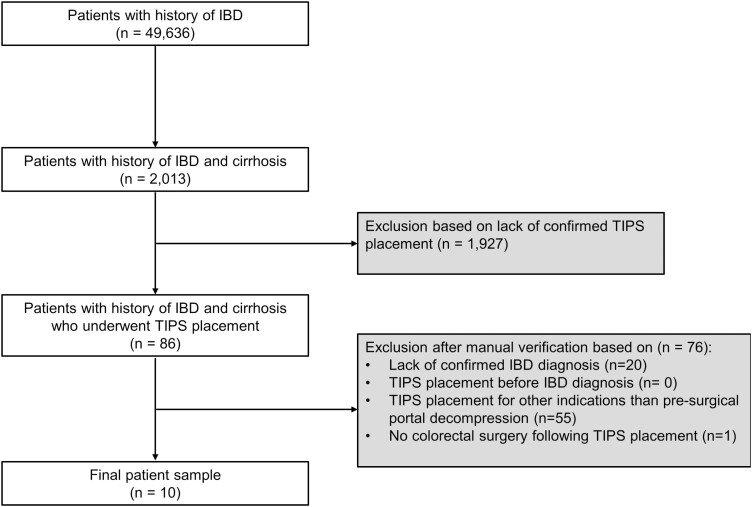
Methods: We identified patients with IBD and cirrhosis who had undergone preoperative TIPS for portal decompression between 2010 and 2023. All other indications for TIPS led to patient exclusion. Demographic and medical data were collected, including portal pressure measurements. Primary outcome of interest was perioperative outcomes.
Results: Ten patients met the inclusion criteria. The most common surgical indications were dysplasia (50%) and refractory IBD (50%). TIPS was performed at a median of 47 days (IQR 34-80) before surgery, with reduction in portal pressures (22.5 vs. 18.5 mmHg, P < .01) and portosystemic gradient (12.5 vs. 5.5 mmHg, P < .01). Perioperative complications occurred in 80% of patients, including surgical site bleeding (30%), wound dehiscence (10%), systemic infection (30%), liver function elevation (50%), and coagulopathy (50%). No patients required re-operation, with median length of stay being 7 days (IQR 5.5-9.3). The 30-day readmission rate was 40%, most commonly for infection (75%), with 2 patients having intra-abdominal abscesses and 1 patient with concern for bowel ischemia. Ninety-day and one-year survival was 100% and 90%, respectively. Patients with primary sclerosing cholangitis (PSC)-cirrhosis were noted to have higher perioperative morbidity and a 30-day readmission rate.
Conclusions: In patients with IBD and cirrhosis, preoperative TIPS facilitated successful surgical intervention despite heightened risk. Nevertheless, significant complications were noted, in particular for patients with PSC-cirrhosis.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
