Georgios Tribonias, Magdalini Velegraki, Maria Tzouvala, Maria Fragaki, Pinelopi Nikolaou, Nikolaos Leontidis, Despoina Arna, Andreas Psistakis, Georgia Mpellou, Maria Palatianou, Ioannis Psaroudakis, Antonios Neokleous, Gregorios Paspatis
{"title":"采用混合内窥镜方法治疗无移位征象的复杂结直肠息肉:希腊的经验。","authors":"Georgios Tribonias, Magdalini Velegraki, Maria Tzouvala, Maria Fragaki, Pinelopi Nikolaou, Nikolaos Leontidis, Despoina Arna, Andreas Psistakis, Georgia Mpellou, Maria Palatianou, Ioannis Psaroudakis, Antonios Neokleous, Gregorios Paspatis","doi":"10.20524/aog.2024.0887","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hybrid approaches combining endoscopic full-thickness resection (EFTR) with conventional techniques (endoscopic mucosal resection [EMR], endoscopic submucosal dissection [ESD]) have enabled the resection of difficult fibrotic colorectal adenomas exhibiting a \"non-lifting\" sign, and polyps in difficult positions. We present our cohort treated with either EMR+EFTR or ESD+EFTR as salvage hybrid endoscopic approaches for complex colorectal polyps not amenable to conventional techniques.</p><p><strong>Methods: </strong>Retrospective analysis included technical success, histological confirmation of margin-free resection, assessment of adverse events and follow up with histological assessment. All patients underwent follow-up endoscopy at least 6 and 12 months post-resection.</p><p><strong>Results: </strong>Fourteen patients underwent hybrid EFTR procedures (11 EMR+EFTR and 3 ESD+EFTR). Technical success was achieved in all cases where the full-thickness resection device (FTRD) was advanced to the site of the resection (100%). In 2 cases, the FTRD system could not be passed through the sigmoid colon because of severe chronic diverticulitis, subsequent fibrosis and stiffness. The mean lesion size in the EMR+EFTR group (41.7 mm; range 20-50 mm) was larger than the ESD+EFTR group (31.7 mm; range 30-35 mm). Six patients (42.9%) were histologically diagnosed with T1 carcinoma. The mean duration of hospitalization was 1.4 days. Follow-up endoscopy was available in all patients and no recurrence was observed with histological confirmation during a mean follow-up period of 15.4 months.</p><p><strong>Conclusion: </strong>Hybrid procedures appear to be safe and effective treatments for complex colorectal lesions not amenable to EMR, ESD or EFTR alone, because of the lesion size, positive non-lifting sign, and difficult positions.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 4","pages":"476-484"},"PeriodicalIF":2.2000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11226737/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hybrid endoscopic approaches for complex colorectal polyps with a non-lifting sign: the Greek experience.\",\"authors\":\"Georgios Tribonias, Magdalini Velegraki, Maria Tzouvala, Maria Fragaki, Pinelopi Nikolaou, Nikolaos Leontidis, Despoina Arna, Andreas Psistakis, Georgia Mpellou, Maria Palatianou, Ioannis Psaroudakis, Antonios Neokleous, Gregorios Paspatis\",\"doi\":\"10.20524/aog.2024.0887\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hybrid approaches combining endoscopic full-thickness resection (EFTR) with conventional techniques (endoscopic mucosal resection [EMR], endoscopic submucosal dissection [ESD]) have enabled the resection of difficult fibrotic colorectal adenomas exhibiting a \\\"non-lifting\\\" sign, and polyps in difficult positions. We present our cohort treated with either EMR+EFTR or ESD+EFTR as salvage hybrid endoscopic approaches for complex colorectal polyps not amenable to conventional techniques.</p><p><strong>Methods: </strong>Retrospective analysis included technical success, histological confirmation of margin-free resection, assessment of adverse events and follow up with histological assessment. All patients underwent follow-up endoscopy at least 6 and 12 months post-resection.</p><p><strong>Results: </strong>Fourteen patients underwent hybrid EFTR procedures (11 EMR+EFTR and 3 ESD+EFTR). Technical success was achieved in all cases where the full-thickness resection device (FTRD) was advanced to the site of the resection (100%). In 2 cases, the FTRD system could not be passed through the sigmoid colon because of severe chronic diverticulitis, subsequent fibrosis and stiffness. The mean lesion size in the EMR+EFTR group (41.7 mm; range 20-50 mm) was larger than the ESD+EFTR group (31.7 mm; range 30-35 mm). Six patients (42.9%) were histologically diagnosed with T1 carcinoma. The mean duration of hospitalization was 1.4 days. Follow-up endoscopy was available in all patients and no recurrence was observed with histological confirmation during a mean follow-up period of 15.4 months.</p><p><strong>Conclusion: </strong>Hybrid procedures appear to be safe and effective treatments for complex colorectal lesions not amenable to EMR, ESD or EFTR alone, because of the lesion size, positive non-lifting sign, and difficult positions.</p>\",\"PeriodicalId\":7978,\"journal\":{\"name\":\"Annals of Gastroenterology\",\"volume\":\"37 4\",\"pages\":\"476-484\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11226737/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20524/aog.2024.0887\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0887","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Hybrid endoscopic approaches for complex colorectal polyps with a non-lifting sign: the Greek experience.
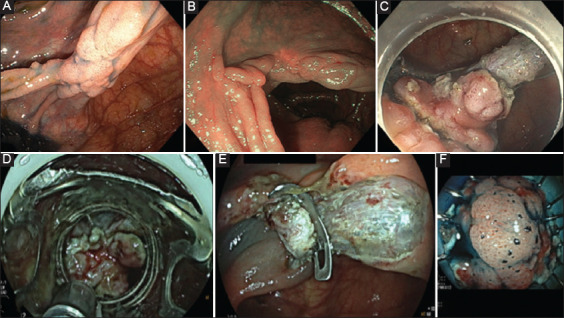
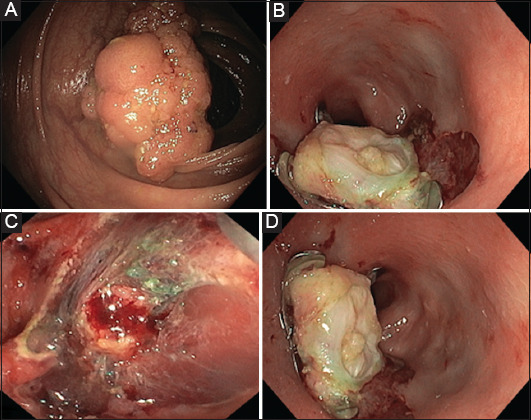
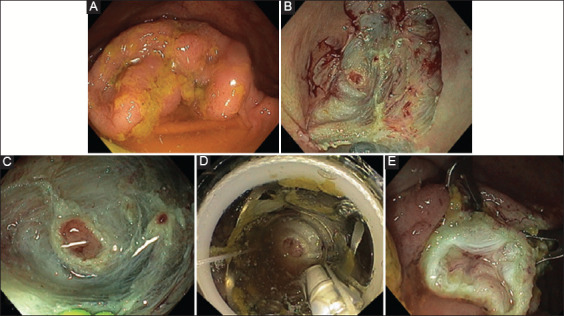
Background: Hybrid approaches combining endoscopic full-thickness resection (EFTR) with conventional techniques (endoscopic mucosal resection [EMR], endoscopic submucosal dissection [ESD]) have enabled the resection of difficult fibrotic colorectal adenomas exhibiting a "non-lifting" sign, and polyps in difficult positions. We present our cohort treated with either EMR+EFTR or ESD+EFTR as salvage hybrid endoscopic approaches for complex colorectal polyps not amenable to conventional techniques.
Methods: Retrospective analysis included technical success, histological confirmation of margin-free resection, assessment of adverse events and follow up with histological assessment. All patients underwent follow-up endoscopy at least 6 and 12 months post-resection.
Results: Fourteen patients underwent hybrid EFTR procedures (11 EMR+EFTR and 3 ESD+EFTR). Technical success was achieved in all cases where the full-thickness resection device (FTRD) was advanced to the site of the resection (100%). In 2 cases, the FTRD system could not be passed through the sigmoid colon because of severe chronic diverticulitis, subsequent fibrosis and stiffness. The mean lesion size in the EMR+EFTR group (41.7 mm; range 20-50 mm) was larger than the ESD+EFTR group (31.7 mm; range 30-35 mm). Six patients (42.9%) were histologically diagnosed with T1 carcinoma. The mean duration of hospitalization was 1.4 days. Follow-up endoscopy was available in all patients and no recurrence was observed with histological confirmation during a mean follow-up period of 15.4 months.
Conclusion: Hybrid procedures appear to be safe and effective treatments for complex colorectal lesions not amenable to EMR, ESD or EFTR alone, because of the lesion size, positive non-lifting sign, and difficult positions.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
