Parth Patel, Bekure B Siraw, Abdulrahim Yusuf Mehadi, Eli Adrian Zaher, Mohamed Ayman Ebrahim, Yordanos T Tafesse
{"title":"憩室出血患者院内预后的预测因素:全国住院患者抽样数据(2016-2020 年)回顾性分析。","authors":"Parth Patel, Bekure B Siraw, Abdulrahim Yusuf Mehadi, Eli Adrian Zaher, Mohamed Ayman Ebrahim, Yordanos T Tafesse","doi":"10.20524/aog.2024.0896","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diverticular bleeding is the leading cause of lower gastrointestinal bleeding, affecting 3-5% of patients with diverticulosis. Current management protocols include resuscitation, diagnosis via direct visualization, computed tomography imaging, endoscopic interventions, angioembolization, and surgery when needed. However, predictive factors for outcomes and optimal interventions remain ambiguous.</p><p><strong>Methods: </strong>This retrospective cohort study analyzed data from the National Inpatient Sample (NIS) database (2016-2020) to determine predictors of adverse in-hospital outcomes in diverticular bleeding patients without perforation or abscess. Demographic and clinical data were extracted, and multivariate regression models were applied. Analysis was conducted using R statistical software (version 4.1.3), with significance set at P<0.05.</p><p><strong>Results: </strong>A total of 28,269 patients hospitalized for diverticular bleeding were identified. Age >85 years, moderate to severe Charlson Comorbidity Index, hypovolemic shock, blood transfusion requirement, and requirement for colectomy were significantly associated with greater in-hospital mortality. Factors such as late colonoscopy timing and colon resection led to longer hospital stays, while arterial embolization was predicted by older age, Black race, hypovolemic shock, and blood transfusion. Predictors of colon resection included advanced age, presence of colon cancer, and hypovolemic shock.</p><p><strong>Conclusions: </strong>Our retrospective study identified significant predictors of in-hospital outcomes among patients with diverticular bleeding, informing risk stratification and management strategies. Further research is warranted to validate these findings and refine management algorithms for improved patient care. Integrating these insights into clinical practice may enhance outcomes and guide personalized interventions in diverticular bleeding management.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 4","pages":"449-457"},"PeriodicalIF":2.2000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11226741/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictors of in-hospital outcomes for diverticular bleeding patients: a retrospective analysis of National Inpatient Sample data (2016-2020).\",\"authors\":\"Parth Patel, Bekure B Siraw, Abdulrahim Yusuf Mehadi, Eli Adrian Zaher, Mohamed Ayman Ebrahim, Yordanos T Tafesse\",\"doi\":\"10.20524/aog.2024.0896\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Diverticular bleeding is the leading cause of lower gastrointestinal bleeding, affecting 3-5% of patients with diverticulosis. Current management protocols include resuscitation, diagnosis via direct visualization, computed tomography imaging, endoscopic interventions, angioembolization, and surgery when needed. However, predictive factors for outcomes and optimal interventions remain ambiguous.</p><p><strong>Methods: </strong>This retrospective cohort study analyzed data from the National Inpatient Sample (NIS) database (2016-2020) to determine predictors of adverse in-hospital outcomes in diverticular bleeding patients without perforation or abscess. Demographic and clinical data were extracted, and multivariate regression models were applied. Analysis was conducted using R statistical software (version 4.1.3), with significance set at P<0.05.</p><p><strong>Results: </strong>A total of 28,269 patients hospitalized for diverticular bleeding were identified. Age >85 years, moderate to severe Charlson Comorbidity Index, hypovolemic shock, blood transfusion requirement, and requirement for colectomy were significantly associated with greater in-hospital mortality. Factors such as late colonoscopy timing and colon resection led to longer hospital stays, while arterial embolization was predicted by older age, Black race, hypovolemic shock, and blood transfusion. Predictors of colon resection included advanced age, presence of colon cancer, and hypovolemic shock.</p><p><strong>Conclusions: </strong>Our retrospective study identified significant predictors of in-hospital outcomes among patients with diverticular bleeding, informing risk stratification and management strategies. Further research is warranted to validate these findings and refine management algorithms for improved patient care. Integrating these insights into clinical practice may enhance outcomes and guide personalized interventions in diverticular bleeding management.</p>\",\"PeriodicalId\":7978,\"journal\":{\"name\":\"Annals of Gastroenterology\",\"volume\":\"37 4\",\"pages\":\"449-457\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11226741/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20524/aog.2024.0896\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0896","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Predictors of in-hospital outcomes for diverticular bleeding patients: a retrospective analysis of National Inpatient Sample data (2016-2020).
Background: Diverticular bleeding is the leading cause of lower gastrointestinal bleeding, affecting 3-5% of patients with diverticulosis. Current management protocols include resuscitation, diagnosis via direct visualization, computed tomography imaging, endoscopic interventions, angioembolization, and surgery when needed. However, predictive factors for outcomes and optimal interventions remain ambiguous.
Methods: This retrospective cohort study analyzed data from the National Inpatient Sample (NIS) database (2016-2020) to determine predictors of adverse in-hospital outcomes in diverticular bleeding patients without perforation or abscess. Demographic and clinical data were extracted, and multivariate regression models were applied. Analysis was conducted using R statistical software (version 4.1.3), with significance set at P<0.05.
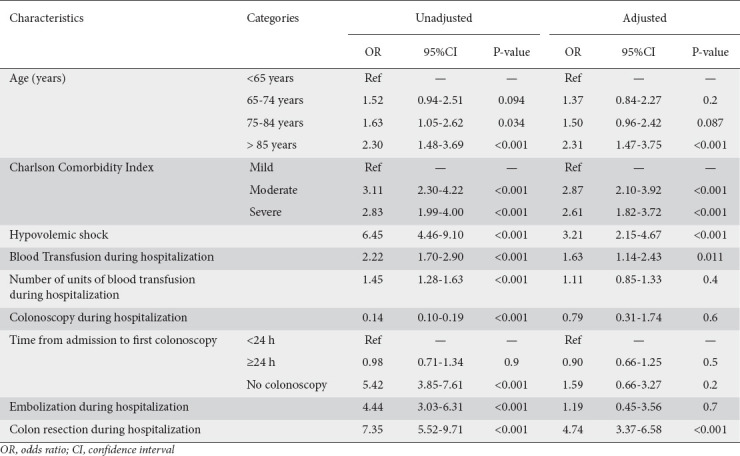
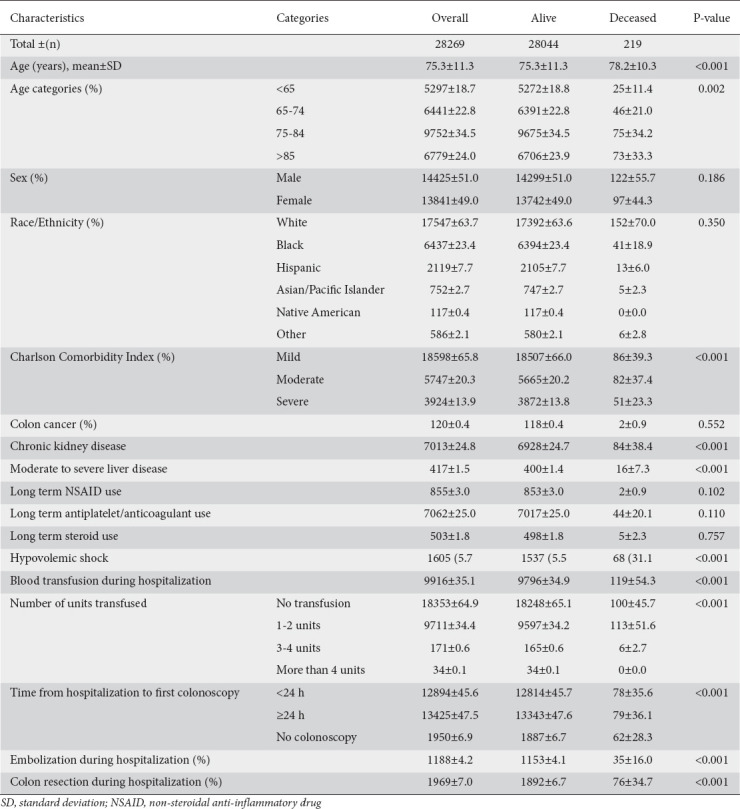
Results: A total of 28,269 patients hospitalized for diverticular bleeding were identified. Age >85 years, moderate to severe Charlson Comorbidity Index, hypovolemic shock, blood transfusion requirement, and requirement for colectomy were significantly associated with greater in-hospital mortality. Factors such as late colonoscopy timing and colon resection led to longer hospital stays, while arterial embolization was predicted by older age, Black race, hypovolemic shock, and blood transfusion. Predictors of colon resection included advanced age, presence of colon cancer, and hypovolemic shock.
Conclusions: Our retrospective study identified significant predictors of in-hospital outcomes among patients with diverticular bleeding, informing risk stratification and management strategies. Further research is warranted to validate these findings and refine management algorithms for improved patient care. Integrating these insights into clinical practice may enhance outcomes and guide personalized interventions in diverticular bleeding management.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
