Antônio da Silva Menezes Júnior, Izadora Caiado Oliveira, André Maroccolo de Sousa, Ricardo Figueiredo Paro Piai, Vinícius Martins Rodrigues Oliveira
{"title":"肥厚型心肌病中皮下与经静脉植入式心律转复除颤器的比较:系统回顾和荟萃分析。","authors":"Antônio da Silva Menezes Júnior, Izadora Caiado Oliveira, André Maroccolo de Sousa, Ricardo Figueiredo Paro Piai, Vinícius Martins Rodrigues Oliveira","doi":"10.21037/cdt-24-15","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A subcutaneous implantable cardioverter-defibrillator (S-ICD) is an alternative to a transvenous implantable cardio defibrillator (TV-ICD). An S-ICD reduces the risk of transvenous lead placement. However, further research is required to determine how S-ICDs affect patients with hypertrophic cardiomyopathy (HCM). In this study, we investigated the comparative efficacy and safety of S-ICDs versus TV-ICDs in HCM.</p><p><strong>Methods: </strong>On December 6<sup>th</sup>, 2023, we performed a comprehensive search of the PubMed, Embase, Scopus, and Cochrane databases to identify randomized clinical trials (RCTs) and observational studies comparing S-ICDs with TV-ICDs in HCM patients published from 2004 until 2023. No language restrictions were applied. The primary outcome was appropriate shocks (AS), with inappropriate shocks (IAS), and device-related complications considered as secondary outcomes. Odds ratios (ORs) and 95% confidence intervals (CIs) were pooled using a random effects model. The ROBINS-I tool was used to assess the risk of bias of the studies.</p><p><strong>Results: </strong>The search yielded 1,114 records. Seven studies comprising 4,347 HCM patients were included, of whom 3,325 (76.0%) had TV-ICDs, and 1,022 (22.6%) had S-ICDs. There were 2,564 males (58.9%). The age range was from 39.1 to 49.4 years. Compared with the TV-ICD group, the S-ICD cohort had a significantly lower incidence of device-related complications (OR 0.52; 95% CI: 0.30-0.89; P=0.02; I<sup>2</sup>=4%). Contrastingly, there were no statistically significant differences in the occurrences of AS (OR 0.49; 95% CI: 0.22-1.08; P=0.08; I<sup>2</sup>=75%) and IAS (OR 1.03; 95% CI: 0.57-1.84; P=0.93; I<sup>2</sup>=65%) between the two device modalities. In the analysis of the overall risk of bias in the studies, we found 42% of them with several, 28% with moderate, and 14% with low risk of bias.</p><p><strong>Conclusions: </strong>In HCM patients, S-ICDs were associated with a lower incidence of device-associated problems than TV-ICDs. AS and IAS incidence rates were similar between groups. These findings may assist clinicians in determining the most suitable device for treating patients with HCM.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"14 3","pages":"318-327"},"PeriodicalIF":2.1000,"publicationDate":"2024-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11223932/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subcutaneous versus transvenous implantable cardioverter defibrillator in hypertrophic cardiomyopathy: a systematic review and meta-analysis.\",\"authors\":\"Antônio da Silva Menezes Júnior, Izadora Caiado Oliveira, André Maroccolo de Sousa, Ricardo Figueiredo Paro Piai, Vinícius Martins Rodrigues Oliveira\",\"doi\":\"10.21037/cdt-24-15\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A subcutaneous implantable cardioverter-defibrillator (S-ICD) is an alternative to a transvenous implantable cardio defibrillator (TV-ICD). An S-ICD reduces the risk of transvenous lead placement. However, further research is required to determine how S-ICDs affect patients with hypertrophic cardiomyopathy (HCM). In this study, we investigated the comparative efficacy and safety of S-ICDs versus TV-ICDs in HCM.</p><p><strong>Methods: </strong>On December 6<sup>th</sup>, 2023, we performed a comprehensive search of the PubMed, Embase, Scopus, and Cochrane databases to identify randomized clinical trials (RCTs) and observational studies comparing S-ICDs with TV-ICDs in HCM patients published from 2004 until 2023. No language restrictions were applied. The primary outcome was appropriate shocks (AS), with inappropriate shocks (IAS), and device-related complications considered as secondary outcomes. Odds ratios (ORs) and 95% confidence intervals (CIs) were pooled using a random effects model. The ROBINS-I tool was used to assess the risk of bias of the studies.</p><p><strong>Results: </strong>The search yielded 1,114 records. Seven studies comprising 4,347 HCM patients were included, of whom 3,325 (76.0%) had TV-ICDs, and 1,022 (22.6%) had S-ICDs. There were 2,564 males (58.9%). The age range was from 39.1 to 49.4 years. Compared with the TV-ICD group, the S-ICD cohort had a significantly lower incidence of device-related complications (OR 0.52; 95% CI: 0.30-0.89; P=0.02; I<sup>2</sup>=4%). Contrastingly, there were no statistically significant differences in the occurrences of AS (OR 0.49; 95% CI: 0.22-1.08; P=0.08; I<sup>2</sup>=75%) and IAS (OR 1.03; 95% CI: 0.57-1.84; P=0.93; I<sup>2</sup>=65%) between the two device modalities. In the analysis of the overall risk of bias in the studies, we found 42% of them with several, 28% with moderate, and 14% with low risk of bias.</p><p><strong>Conclusions: </strong>In HCM patients, S-ICDs were associated with a lower incidence of device-associated problems than TV-ICDs. AS and IAS incidence rates were similar between groups. These findings may assist clinicians in determining the most suitable device for treating patients with HCM.</p>\",\"PeriodicalId\":9592,\"journal\":{\"name\":\"Cardiovascular diagnosis and therapy\",\"volume\":\"14 3\",\"pages\":\"318-327\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11223932/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiovascular diagnosis and therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/cdt-24-15\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-24-15","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/27 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Subcutaneous versus transvenous implantable cardioverter defibrillator in hypertrophic cardiomyopathy: a systematic review and meta-analysis.
Background: A subcutaneous implantable cardioverter-defibrillator (S-ICD) is an alternative to a transvenous implantable cardio defibrillator (TV-ICD). An S-ICD reduces the risk of transvenous lead placement. However, further research is required to determine how S-ICDs affect patients with hypertrophic cardiomyopathy (HCM). In this study, we investigated the comparative efficacy and safety of S-ICDs versus TV-ICDs in HCM.
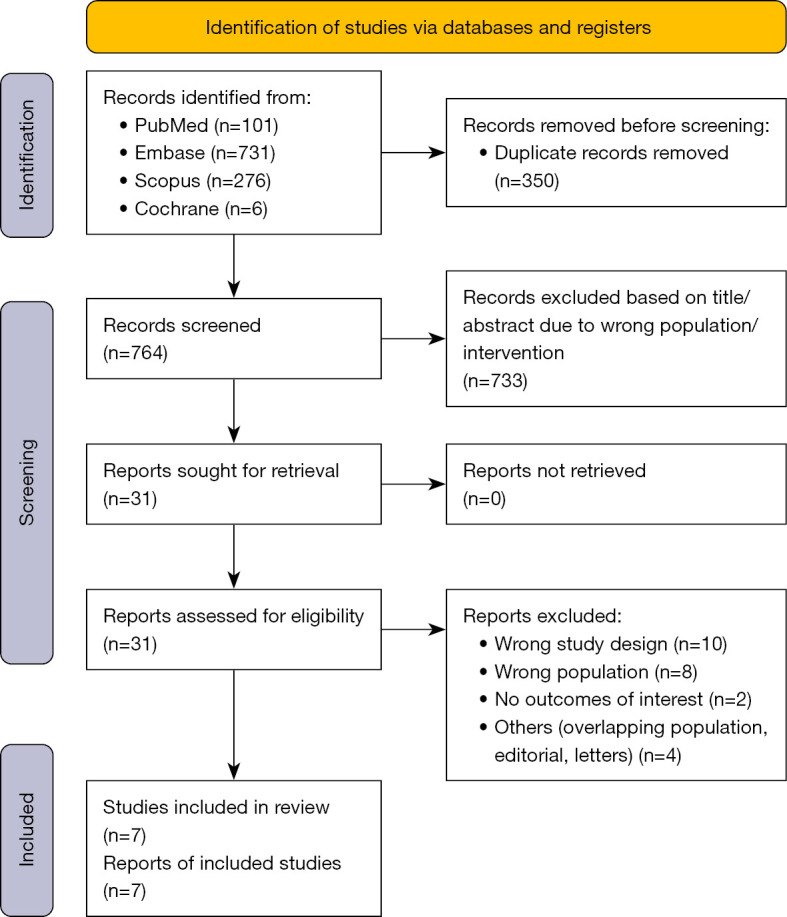
Methods: On December 6th, 2023, we performed a comprehensive search of the PubMed, Embase, Scopus, and Cochrane databases to identify randomized clinical trials (RCTs) and observational studies comparing S-ICDs with TV-ICDs in HCM patients published from 2004 until 2023. No language restrictions were applied. The primary outcome was appropriate shocks (AS), with inappropriate shocks (IAS), and device-related complications considered as secondary outcomes. Odds ratios (ORs) and 95% confidence intervals (CIs) were pooled using a random effects model. The ROBINS-I tool was used to assess the risk of bias of the studies.
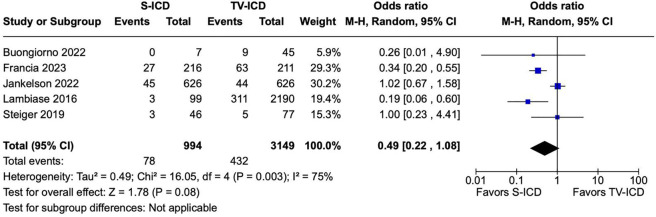
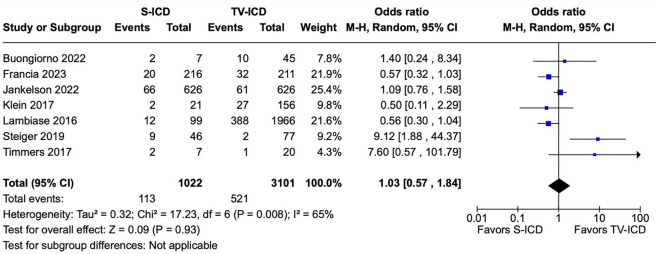
Results: The search yielded 1,114 records. Seven studies comprising 4,347 HCM patients were included, of whom 3,325 (76.0%) had TV-ICDs, and 1,022 (22.6%) had S-ICDs. There were 2,564 males (58.9%). The age range was from 39.1 to 49.4 years. Compared with the TV-ICD group, the S-ICD cohort had a significantly lower incidence of device-related complications (OR 0.52; 95% CI: 0.30-0.89; P=0.02; I2=4%). Contrastingly, there were no statistically significant differences in the occurrences of AS (OR 0.49; 95% CI: 0.22-1.08; P=0.08; I2=75%) and IAS (OR 1.03; 95% CI: 0.57-1.84; P=0.93; I2=65%) between the two device modalities. In the analysis of the overall risk of bias in the studies, we found 42% of them with several, 28% with moderate, and 14% with low risk of bias.
Conclusions: In HCM patients, S-ICDs were associated with a lower incidence of device-associated problems than TV-ICDs. AS and IAS incidence rates were similar between groups. These findings may assist clinicians in determining the most suitable device for treating patients with HCM.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
