Shuqui Qin, Jin Li, Aiping Zhou, Yanqiao Zhang, Xianglin Yuan, Liangjun Zhu, Baoli Qin, Shan Zeng, Lin Shen, Ying Yuan, Weibo Wang, Jun Liang, Xianwen Zhang, Feng Ye, Ping Chen, Huaizhang Wang, Zhenyan Yu, Lu Yue, Yong Fang, Jianping Xiong, Jianwei Yang, Yiye Wan, Xianli Yin, Wenling Wang, Nong Xu, Xiaohong Wang, Zemin Xiao, Huafang Su, Ying Wang, Kangsheng Gu, Shuiping Tu, Zishu Wang, Bo Liu, Xiaohua Hu, Weixian Liu, Xiaofeng Li
{"title":"将基于 SALIRI(拉替曲塞加伊立替康)的疗法作为转移性结直肠癌患者的二线治疗方法(SALLY):一项前瞻性、多中心、非干预性登记研究。","authors":"Shuqui Qin, Jin Li, Aiping Zhou, Yanqiao Zhang, Xianglin Yuan, Liangjun Zhu, Baoli Qin, Shan Zeng, Lin Shen, Ying Yuan, Weibo Wang, Jun Liang, Xianwen Zhang, Feng Ye, Ping Chen, Huaizhang Wang, Zhenyan Yu, Lu Yue, Yong Fang, Jianping Xiong, Jianwei Yang, Yiye Wan, Xianli Yin, Wenling Wang, Nong Xu, Xiaohong Wang, Zemin Xiao, Huafang Su, Ying Wang, Kangsheng Gu, Shuiping Tu, Zishu Wang, Bo Liu, Xiaohua Hu, Weixian Liu, Xiaofeng Li","doi":"10.1002/cac2.12586","DOIUrl":null,"url":null,"abstract":"<p>Primary chemotherapy options for colorectal cancer (CRC) involve four key drugs: fluorouracils (5-FU), oxaliplatin, irinotecan and raltitrexed. The first-line regimen consists of 5-FU and leucovorin combined with oxaliplatin (FOLFOX), while the second-line regimen involves 5-FU and leucovorin combined with irinotecan (FOLFIRI) for metastatic CRC (mCRC) in China [<span>1</span>]. Efficacy findings for FOLFOX and FOLFIRI as first-line treatments reported overall response rates (ORRs) of 54% and 56%, with median progression-free survival (mPFS) of 8.0 and 8.5 months, respectively. In the second-line setting, ORRs decreased to 15% and 4%, with mPFS of 4.2 and 2.5 months, respectively, possibly indicating induced drug resistance due to repeated 5-FU infusions in both first-line and second-line treatments [<span>2</span>]. Our present research was a prospective, non-interventional clinical trial conducted in 58 centers across China. The design and procedures are shown in the Supplementary Material. From April 2018 to March 2021, a total of 1,067 mCRC patients were enrolled for second-line treatment with raltitrexed plus irinotecan (SALIRI regimen) following unsuccessful 5-FU combined with platinum-based drug treatment, of whom 1,066 were included in the full analysis set (FAS) and 1,042 in the per-protocol set (PPS). The demographics, baseline and clinical characteristics of the patients are detailed in Supplementary Table S1.</p><p>The primary outcome revealed a mPFS of 7.3 months (range: 0.8-40.7, 95% confidence interval [CI]: 7.0-7.6) and a median overall survival (mOS) of 17.8 months (range: 1.4-47.3, 95% CI: 17.0-19.2) in both the FAS and PPS cohorts (Figure 1A-D, Supplementary Table S2).</p><p>Regarding secondary outcomes, mPFS and mOS were 5.8 (range: 0.8-34.5) and 17.0 (range: 1.8-47.3) months in the SALIRI group (<i>n</i> = 268), whereas in the SALIRI + targeted therapy (TAR; <i>n</i> = 795), including cetuximab (<i>n</i> = 103), bevacizumab (<i>n</i> = 678) or post-cetuximab + bevacizumab (<i>n</i> = 9) or the other targeted drug group (<i>n</i> = 5), mPFS and mOS were 7.6 (range: 0.8-40.7) and 18.1 (range: 1.4-40.7) months. A significant difference only in OS was found between SALIRI and the SALIRI + TAR groups (<i>P</i> = 0.045) (Figure 1E-F).</p><p>Subsequently, the ORR and disease control rate (DCR) for the entire cohort were 19.5% and 84.2%, respectively. The best tumor response comprised 1 patient achieving a complete response (0.1%), 207 with partial responses (19.4%), 690 attaining stable disease (64.7%) and 144 experiencing progressive disease (13.5%). However, in the SALIRI + TAR group, the ORR and DCR were 20.9% (95% CI: 18.1-23.9) and 85.8% (95% CI: 83.2-88.1), whereas in the SALIRI group, the ORR and DCR were 15.7% (95% CI: 11.5-20.6) and 80.6% (95% CI: 75.4-85.2), respectively (Supplementary Table S2).</p><p>In addition, an exploration of PFS and OS among patients with diverse genotypes, including mutation states of rat sarcoma viral oncogene homolog <i>(RAS)</i>, v-raf murine sarcoma viral oncogene homolog B1 <i>(BRAF)</i> and microsatellite stability (MSS)/high microsatellite instability (MSI-H), was conducted. MSS/MSI-H status was measured by immunohistochemistry (IHC) or the capillary electrophoresis-based multiplex polymerase chain reaction. The measurements of other genotype mutation states are described in the Supplementary Material. Patients with <i>RAS</i> mutations exhibited a comparatively shorter mPFS of 7.1 months (range: 1.1-22.1, 95% CI: 6.5-7.7), while those with the <i>RAS</i> wild-type had a mPFS of 7.8 months (range: 0.9-32.6, 95% CI: 7.1-8.2). The mPFS for patients with <i>BRAF</i> mutations was 5.4 months (range: 1.9-19.4, 95% CI: 2.6-12.1), in contrast to 7.4 months (range: 0.9-32.6, 95% CI: 6.8–7.8) for the <i>BRAF</i> wild-type. Similarly, it was also shown that the mOS of patients with <i>RAS</i> mutations was 16.4 months (range: 1.4-38.7, 95% CI: 14.4-18.9), while those with the <i>RAS</i> wild-type appeared to have a relatively longer mOS time of 19.4 months (range: 1.8-36.9, 95% CI: 17.0-21.2),. The mOS for patients with <i>BRAF</i> mutations was 18.1 months (range: 5.7-22.7, 95% CI: 6.5-22.7) compared to 17.7 months (range: 1.8-38.7, 95% CI: 16.4-19.7) for the wild-type. However, all apparent differences between the mutations and wild-type groups were not statistically significant. In the subgroup analysis, for MSS/mismatch repair proficient (pMMR) mCRC patients who received SALIRI-based therapy, the mPFS was 7.7 months (range: 0.9-28.6, 95% CI: 7.1-8.0) and for those with MSI-H-related cases, it was 7.8 months (range: 2.0-14.3, 95% CI: 5.3-11.6). MSS/pMMR- or MSI-H-related mOS in mCRC patients were 18.1 months (range: 2.4-39.6, 95% CI: 16.3-19.9) and 19.9 months (range: 3.4-20.6, 95% CI: 5.3–not evaluable), respectively (Supplementary Table S3).</p><p>These findings contradict the prevailing reports that 95% of MSS/pMMR CRC patients exhibit poor responses to immune checkpoint inhibitors [<span>3</span>] and demonstrate that SALIRI-based treatment approaches may represent a promising option for managing MSS/pMMR CRC. Moreover, only 14 patients (1.3%) were identified as MSI-H in the present trial, and 711 (66.7%) remained undetermined (Supplementary Table S1), possibly due to limitations in current MSI-H status identification methods. Typically, IHC provides widely accessible protein expression analysis but necessitates high-quality tissue samples. MSI-H polymerase chain reaction analysis can evaluate specific microsatellite loci, albeit at a higher cost. Therefore, enhancing the capacity to detect accurately the MSI-H patient status in the future is paramount.</p><p>Furthermore, the analysis of risk factors for mPFS and mOS after treatment revealed significant correlations between excision of the primary site and mPFS and mOS as well as addition of TAR to SALIRI and mOS times. Age, gender or the primary tumor site location were not potential risk factors for mPFS and mOS of the patients (Supplementary Table S4).</p><p>In the present study, 5-FU and oxaliplatin were exchanged with SALIRI, which led to a series of outcomes in the real-life setting (mPFS and mOS of 7.3 and 17.8 months, an ORR of 19.5% and DCR of 84.2%). Compared with irinotecan monotherapy [<span>4</span>], the FOLFIRI regimen [<span>4-6</span>] and the regimen comprising capecitabine plus irinotecan (XELIRI) [<span>7</span>], the present outcomes may validate the problem of repeated use resistance to 5-FU-based regimens with raltitrexed as an alternative treatment for continued 5-FU application from a clinical point of view. In addition, mOS and mPFS were prolonged when SALIRI was used in combination with TAR, a finding in good agreement with those reported in previous studies in which the addition of bevacizumab to chemotherapy regimens was shown to be beneficial for mCRC treatment [<span>8-10</span>]. Regarding safety, in the present trial, an average relative dose intensity of 99.7% (SD 3.9%, range: 48.2%–154.5%; relative dose intensity = actual dose intensity / planned dose intensity * 100%) of raltitrexed for SALIRI-based chemotherapy regimens was achieved, and dose adjustment was not required for 80.7% (861/1,067) of patients in their overall treatment regimens. There were 13.1% (140/1,067) grade III/IV adverse events (AEs) and 7.2% (77/1,067) AEs which led to raltitrexed dose reductions or drug discontinuation, but no AEs were fatal (Supplementary Tables S5-S6). Raltitrexed requires only a 15-min intravenous infusion for its administration, which improves patient compliance compared to oral medication problems, such as misuse, missed doses or multiple doses. In addition, due to its safety profile, some patients can complete their treatment on the day ward, thereby improving their quality of life. An advantage of the present study was its prospective design, over a wide range of Chinese regions that included patients aged from 20 years to 80 years regardless of <i>RAS</i> genotype and thus, the results are likely to be representative of the overall Chinese population.</p><p>In summary, exchanging 5-FU and oxaliplatin with SALIRI after first-line chemotherapy led to favorable mPFS and mOS, especially when combined with targeted drugs for the treatment of mCRC, which may solve the problem of repeated use resistance to 5-FU analogs and thus improve therapeutic outcomes.</p><p><i>Conceptualization</i>: Shuqui Qin and Jin Li. <i>Formal analysis</i>: All authors. <i>Investigation</i>: All authors. <i>Writing—original draft</i>: Shuqui Qin and Jin Li. <i>Writing—review & editing</i>: All authors. <i>Manuscript approval</i>: All authors. <i>Supervision</i>: Jin Li. <i>Project administration</i>: Jin Li.</p><p>The authors declare no conflict of interest.</p><p>None.</p><p>The trial was in accordance with the Helsinki Declaration and was approved by the ethics committees of Tongji University Shanghai East Hospital (approval number: 2018-Research Review No. 12) and Bayi Hospital Nanjing Chinese Medicine University (approval number: 81YY-ZLLL-17-32). All patients signed informed consent forms. This study was registered with the Chinese Clinical Trial Registry (registration number: ChiCTR1800016185).</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 8","pages":"910-914"},"PeriodicalIF":24.9000,"publicationDate":"2024-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12586","citationCount":"0","resultStr":"{\"title\":\"SALIRI-based (raltitrexed plus irinotecan) therapy as a second-line treatment for patients with metastatic colorectal cancer (SALLY): A prospective, multicenter, non-interventional, registry study\",\"authors\":\"Shuqui Qin, Jin Li, Aiping Zhou, Yanqiao Zhang, Xianglin Yuan, Liangjun Zhu, Baoli Qin, Shan Zeng, Lin Shen, Ying Yuan, Weibo Wang, Jun Liang, Xianwen Zhang, Feng Ye, Ping Chen, Huaizhang Wang, Zhenyan Yu, Lu Yue, Yong Fang, Jianping Xiong, Jianwei Yang, Yiye Wan, Xianli Yin, Wenling Wang, Nong Xu, Xiaohong Wang, Zemin Xiao, Huafang Su, Ying Wang, Kangsheng Gu, Shuiping Tu, Zishu Wang, Bo Liu, Xiaohua Hu, Weixian Liu, Xiaofeng Li\",\"doi\":\"10.1002/cac2.12586\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Primary chemotherapy options for colorectal cancer (CRC) involve four key drugs: fluorouracils (5-FU), oxaliplatin, irinotecan and raltitrexed. The first-line regimen consists of 5-FU and leucovorin combined with oxaliplatin (FOLFOX), while the second-line regimen involves 5-FU and leucovorin combined with irinotecan (FOLFIRI) for metastatic CRC (mCRC) in China [<span>1</span>]. Efficacy findings for FOLFOX and FOLFIRI as first-line treatments reported overall response rates (ORRs) of 54% and 56%, with median progression-free survival (mPFS) of 8.0 and 8.5 months, respectively. In the second-line setting, ORRs decreased to 15% and 4%, with mPFS of 4.2 and 2.5 months, respectively, possibly indicating induced drug resistance due to repeated 5-FU infusions in both first-line and second-line treatments [<span>2</span>]. Our present research was a prospective, non-interventional clinical trial conducted in 58 centers across China. The design and procedures are shown in the Supplementary Material. From April 2018 to March 2021, a total of 1,067 mCRC patients were enrolled for second-line treatment with raltitrexed plus irinotecan (SALIRI regimen) following unsuccessful 5-FU combined with platinum-based drug treatment, of whom 1,066 were included in the full analysis set (FAS) and 1,042 in the per-protocol set (PPS). The demographics, baseline and clinical characteristics of the patients are detailed in Supplementary Table S1.</p><p>The primary outcome revealed a mPFS of 7.3 months (range: 0.8-40.7, 95% confidence interval [CI]: 7.0-7.6) and a median overall survival (mOS) of 17.8 months (range: 1.4-47.3, 95% CI: 17.0-19.2) in both the FAS and PPS cohorts (Figure 1A-D, Supplementary Table S2).</p><p>Regarding secondary outcomes, mPFS and mOS were 5.8 (range: 0.8-34.5) and 17.0 (range: 1.8-47.3) months in the SALIRI group (<i>n</i> = 268), whereas in the SALIRI + targeted therapy (TAR; <i>n</i> = 795), including cetuximab (<i>n</i> = 103), bevacizumab (<i>n</i> = 678) or post-cetuximab + bevacizumab (<i>n</i> = 9) or the other targeted drug group (<i>n</i> = 5), mPFS and mOS were 7.6 (range: 0.8-40.7) and 18.1 (range: 1.4-40.7) months. A significant difference only in OS was found between SALIRI and the SALIRI + TAR groups (<i>P</i> = 0.045) (Figure 1E-F).</p><p>Subsequently, the ORR and disease control rate (DCR) for the entire cohort were 19.5% and 84.2%, respectively. The best tumor response comprised 1 patient achieving a complete response (0.1%), 207 with partial responses (19.4%), 690 attaining stable disease (64.7%) and 144 experiencing progressive disease (13.5%). However, in the SALIRI + TAR group, the ORR and DCR were 20.9% (95% CI: 18.1-23.9) and 85.8% (95% CI: 83.2-88.1), whereas in the SALIRI group, the ORR and DCR were 15.7% (95% CI: 11.5-20.6) and 80.6% (95% CI: 75.4-85.2), respectively (Supplementary Table S2).</p><p>In addition, an exploration of PFS and OS among patients with diverse genotypes, including mutation states of rat sarcoma viral oncogene homolog <i>(RAS)</i>, v-raf murine sarcoma viral oncogene homolog B1 <i>(BRAF)</i> and microsatellite stability (MSS)/high microsatellite instability (MSI-H), was conducted. MSS/MSI-H status was measured by immunohistochemistry (IHC) or the capillary electrophoresis-based multiplex polymerase chain reaction. The measurements of other genotype mutation states are described in the Supplementary Material. Patients with <i>RAS</i> mutations exhibited a comparatively shorter mPFS of 7.1 months (range: 1.1-22.1, 95% CI: 6.5-7.7), while those with the <i>RAS</i> wild-type had a mPFS of 7.8 months (range: 0.9-32.6, 95% CI: 7.1-8.2). The mPFS for patients with <i>BRAF</i> mutations was 5.4 months (range: 1.9-19.4, 95% CI: 2.6-12.1), in contrast to 7.4 months (range: 0.9-32.6, 95% CI: 6.8–7.8) for the <i>BRAF</i> wild-type. Similarly, it was also shown that the mOS of patients with <i>RAS</i> mutations was 16.4 months (range: 1.4-38.7, 95% CI: 14.4-18.9), while those with the <i>RAS</i> wild-type appeared to have a relatively longer mOS time of 19.4 months (range: 1.8-36.9, 95% CI: 17.0-21.2),. The mOS for patients with <i>BRAF</i> mutations was 18.1 months (range: 5.7-22.7, 95% CI: 6.5-22.7) compared to 17.7 months (range: 1.8-38.7, 95% CI: 16.4-19.7) for the wild-type. However, all apparent differences between the mutations and wild-type groups were not statistically significant. In the subgroup analysis, for MSS/mismatch repair proficient (pMMR) mCRC patients who received SALIRI-based therapy, the mPFS was 7.7 months (range: 0.9-28.6, 95% CI: 7.1-8.0) and for those with MSI-H-related cases, it was 7.8 months (range: 2.0-14.3, 95% CI: 5.3-11.6). MSS/pMMR- or MSI-H-related mOS in mCRC patients were 18.1 months (range: 2.4-39.6, 95% CI: 16.3-19.9) and 19.9 months (range: 3.4-20.6, 95% CI: 5.3–not evaluable), respectively (Supplementary Table S3).</p><p>These findings contradict the prevailing reports that 95% of MSS/pMMR CRC patients exhibit poor responses to immune checkpoint inhibitors [<span>3</span>] and demonstrate that SALIRI-based treatment approaches may represent a promising option for managing MSS/pMMR CRC. Moreover, only 14 patients (1.3%) were identified as MSI-H in the present trial, and 711 (66.7%) remained undetermined (Supplementary Table S1), possibly due to limitations in current MSI-H status identification methods. Typically, IHC provides widely accessible protein expression analysis but necessitates high-quality tissue samples. MSI-H polymerase chain reaction analysis can evaluate specific microsatellite loci, albeit at a higher cost. Therefore, enhancing the capacity to detect accurately the MSI-H patient status in the future is paramount.</p><p>Furthermore, the analysis of risk factors for mPFS and mOS after treatment revealed significant correlations between excision of the primary site and mPFS and mOS as well as addition of TAR to SALIRI and mOS times. Age, gender or the primary tumor site location were not potential risk factors for mPFS and mOS of the patients (Supplementary Table S4).</p><p>In the present study, 5-FU and oxaliplatin were exchanged with SALIRI, which led to a series of outcomes in the real-life setting (mPFS and mOS of 7.3 and 17.8 months, an ORR of 19.5% and DCR of 84.2%). Compared with irinotecan monotherapy [<span>4</span>], the FOLFIRI regimen [<span>4-6</span>] and the regimen comprising capecitabine plus irinotecan (XELIRI) [<span>7</span>], the present outcomes may validate the problem of repeated use resistance to 5-FU-based regimens with raltitrexed as an alternative treatment for continued 5-FU application from a clinical point of view. In addition, mOS and mPFS were prolonged when SALIRI was used in combination with TAR, a finding in good agreement with those reported in previous studies in which the addition of bevacizumab to chemotherapy regimens was shown to be beneficial for mCRC treatment [<span>8-10</span>]. Regarding safety, in the present trial, an average relative dose intensity of 99.7% (SD 3.9%, range: 48.2%–154.5%; relative dose intensity = actual dose intensity / planned dose intensity * 100%) of raltitrexed for SALIRI-based chemotherapy regimens was achieved, and dose adjustment was not required for 80.7% (861/1,067) of patients in their overall treatment regimens. There were 13.1% (140/1,067) grade III/IV adverse events (AEs) and 7.2% (77/1,067) AEs which led to raltitrexed dose reductions or drug discontinuation, but no AEs were fatal (Supplementary Tables S5-S6). Raltitrexed requires only a 15-min intravenous infusion for its administration, which improves patient compliance compared to oral medication problems, such as misuse, missed doses or multiple doses. In addition, due to its safety profile, some patients can complete their treatment on the day ward, thereby improving their quality of life. An advantage of the present study was its prospective design, over a wide range of Chinese regions that included patients aged from 20 years to 80 years regardless of <i>RAS</i> genotype and thus, the results are likely to be representative of the overall Chinese population.</p><p>In summary, exchanging 5-FU and oxaliplatin with SALIRI after first-line chemotherapy led to favorable mPFS and mOS, especially when combined with targeted drugs for the treatment of mCRC, which may solve the problem of repeated use resistance to 5-FU analogs and thus improve therapeutic outcomes.</p><p><i>Conceptualization</i>: Shuqui Qin and Jin Li. <i>Formal analysis</i>: All authors. <i>Investigation</i>: All authors. <i>Writing—original draft</i>: Shuqui Qin and Jin Li. <i>Writing—review & editing</i>: All authors. <i>Manuscript approval</i>: All authors. <i>Supervision</i>: Jin Li. <i>Project administration</i>: Jin Li.</p><p>The authors declare no conflict of interest.</p><p>None.</p><p>The trial was in accordance with the Helsinki Declaration and was approved by the ethics committees of Tongji University Shanghai East Hospital (approval number: 2018-Research Review No. 12) and Bayi Hospital Nanjing Chinese Medicine University (approval number: 81YY-ZLLL-17-32). All patients signed informed consent forms. This study was registered with the Chinese Clinical Trial Registry (registration number: ChiCTR1800016185).</p>\",\"PeriodicalId\":9495,\"journal\":{\"name\":\"Cancer Communications\",\"volume\":\"44 8\",\"pages\":\"910-914\"},\"PeriodicalIF\":24.9000,\"publicationDate\":\"2024-07-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12586\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Communications\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12586\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12586","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
SALIRI-based (raltitrexed plus irinotecan) therapy as a second-line treatment for patients with metastatic colorectal cancer (SALLY): A prospective, multicenter, non-interventional, registry study
Primary chemotherapy options for colorectal cancer (CRC) involve four key drugs: fluorouracils (5-FU), oxaliplatin, irinotecan and raltitrexed. The first-line regimen consists of 5-FU and leucovorin combined with oxaliplatin (FOLFOX), while the second-line regimen involves 5-FU and leucovorin combined with irinotecan (FOLFIRI) for metastatic CRC (mCRC) in China [1]. Efficacy findings for FOLFOX and FOLFIRI as first-line treatments reported overall response rates (ORRs) of 54% and 56%, with median progression-free survival (mPFS) of 8.0 and 8.5 months, respectively. In the second-line setting, ORRs decreased to 15% and 4%, with mPFS of 4.2 and 2.5 months, respectively, possibly indicating induced drug resistance due to repeated 5-FU infusions in both first-line and second-line treatments [2]. Our present research was a prospective, non-interventional clinical trial conducted in 58 centers across China. The design and procedures are shown in the Supplementary Material. From April 2018 to March 2021, a total of 1,067 mCRC patients were enrolled for second-line treatment with raltitrexed plus irinotecan (SALIRI regimen) following unsuccessful 5-FU combined with platinum-based drug treatment, of whom 1,066 were included in the full analysis set (FAS) and 1,042 in the per-protocol set (PPS). The demographics, baseline and clinical characteristics of the patients are detailed in Supplementary Table S1.
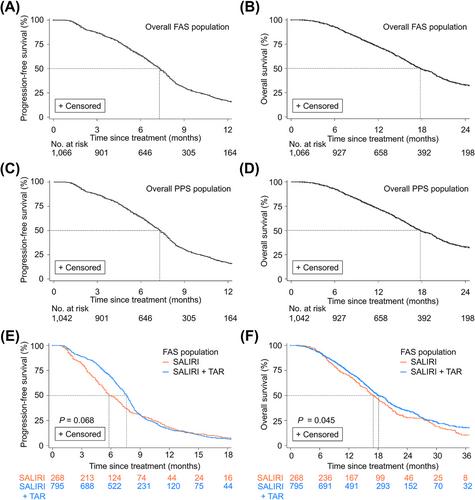
The primary outcome revealed a mPFS of 7.3 months (range: 0.8-40.7, 95% confidence interval [CI]: 7.0-7.6) and a median overall survival (mOS) of 17.8 months (range: 1.4-47.3, 95% CI: 17.0-19.2) in both the FAS and PPS cohorts (Figure 1A-D, Supplementary Table S2).
Regarding secondary outcomes, mPFS and mOS were 5.8 (range: 0.8-34.5) and 17.0 (range: 1.8-47.3) months in the SALIRI group (n = 268), whereas in the SALIRI + targeted therapy (TAR; n = 795), including cetuximab (n = 103), bevacizumab (n = 678) or post-cetuximab + bevacizumab (n = 9) or the other targeted drug group (n = 5), mPFS and mOS were 7.6 (range: 0.8-40.7) and 18.1 (range: 1.4-40.7) months. A significant difference only in OS was found between SALIRI and the SALIRI + TAR groups (P = 0.045) (Figure 1E-F).
Subsequently, the ORR and disease control rate (DCR) for the entire cohort were 19.5% and 84.2%, respectively. The best tumor response comprised 1 patient achieving a complete response (0.1%), 207 with partial responses (19.4%), 690 attaining stable disease (64.7%) and 144 experiencing progressive disease (13.5%). However, in the SALIRI + TAR group, the ORR and DCR were 20.9% (95% CI: 18.1-23.9) and 85.8% (95% CI: 83.2-88.1), whereas in the SALIRI group, the ORR and DCR were 15.7% (95% CI: 11.5-20.6) and 80.6% (95% CI: 75.4-85.2), respectively (Supplementary Table S2).
In addition, an exploration of PFS and OS among patients with diverse genotypes, including mutation states of rat sarcoma viral oncogene homolog (RAS), v-raf murine sarcoma viral oncogene homolog B1 (BRAF) and microsatellite stability (MSS)/high microsatellite instability (MSI-H), was conducted. MSS/MSI-H status was measured by immunohistochemistry (IHC) or the capillary electrophoresis-based multiplex polymerase chain reaction. The measurements of other genotype mutation states are described in the Supplementary Material. Patients with RAS mutations exhibited a comparatively shorter mPFS of 7.1 months (range: 1.1-22.1, 95% CI: 6.5-7.7), while those with the RAS wild-type had a mPFS of 7.8 months (range: 0.9-32.6, 95% CI: 7.1-8.2). The mPFS for patients with BRAF mutations was 5.4 months (range: 1.9-19.4, 95% CI: 2.6-12.1), in contrast to 7.4 months (range: 0.9-32.6, 95% CI: 6.8–7.8) for the BRAF wild-type. Similarly, it was also shown that the mOS of patients with RAS mutations was 16.4 months (range: 1.4-38.7, 95% CI: 14.4-18.9), while those with the RAS wild-type appeared to have a relatively longer mOS time of 19.4 months (range: 1.8-36.9, 95% CI: 17.0-21.2),. The mOS for patients with BRAF mutations was 18.1 months (range: 5.7-22.7, 95% CI: 6.5-22.7) compared to 17.7 months (range: 1.8-38.7, 95% CI: 16.4-19.7) for the wild-type. However, all apparent differences between the mutations and wild-type groups were not statistically significant. In the subgroup analysis, for MSS/mismatch repair proficient (pMMR) mCRC patients who received SALIRI-based therapy, the mPFS was 7.7 months (range: 0.9-28.6, 95% CI: 7.1-8.0) and for those with MSI-H-related cases, it was 7.8 months (range: 2.0-14.3, 95% CI: 5.3-11.6). MSS/pMMR- or MSI-H-related mOS in mCRC patients were 18.1 months (range: 2.4-39.6, 95% CI: 16.3-19.9) and 19.9 months (range: 3.4-20.6, 95% CI: 5.3–not evaluable), respectively (Supplementary Table S3).
These findings contradict the prevailing reports that 95% of MSS/pMMR CRC patients exhibit poor responses to immune checkpoint inhibitors [3] and demonstrate that SALIRI-based treatment approaches may represent a promising option for managing MSS/pMMR CRC. Moreover, only 14 patients (1.3%) were identified as MSI-H in the present trial, and 711 (66.7%) remained undetermined (Supplementary Table S1), possibly due to limitations in current MSI-H status identification methods. Typically, IHC provides widely accessible protein expression analysis but necessitates high-quality tissue samples. MSI-H polymerase chain reaction analysis can evaluate specific microsatellite loci, albeit at a higher cost. Therefore, enhancing the capacity to detect accurately the MSI-H patient status in the future is paramount.
Furthermore, the analysis of risk factors for mPFS and mOS after treatment revealed significant correlations between excision of the primary site and mPFS and mOS as well as addition of TAR to SALIRI and mOS times. Age, gender or the primary tumor site location were not potential risk factors for mPFS and mOS of the patients (Supplementary Table S4).
In the present study, 5-FU and oxaliplatin were exchanged with SALIRI, which led to a series of outcomes in the real-life setting (mPFS and mOS of 7.3 and 17.8 months, an ORR of 19.5% and DCR of 84.2%). Compared with irinotecan monotherapy [4], the FOLFIRI regimen [4-6] and the regimen comprising capecitabine plus irinotecan (XELIRI) [7], the present outcomes may validate the problem of repeated use resistance to 5-FU-based regimens with raltitrexed as an alternative treatment for continued 5-FU application from a clinical point of view. In addition, mOS and mPFS were prolonged when SALIRI was used in combination with TAR, a finding in good agreement with those reported in previous studies in which the addition of bevacizumab to chemotherapy regimens was shown to be beneficial for mCRC treatment [8-10]. Regarding safety, in the present trial, an average relative dose intensity of 99.7% (SD 3.9%, range: 48.2%–154.5%; relative dose intensity = actual dose intensity / planned dose intensity * 100%) of raltitrexed for SALIRI-based chemotherapy regimens was achieved, and dose adjustment was not required for 80.7% (861/1,067) of patients in their overall treatment regimens. There were 13.1% (140/1,067) grade III/IV adverse events (AEs) and 7.2% (77/1,067) AEs which led to raltitrexed dose reductions or drug discontinuation, but no AEs were fatal (Supplementary Tables S5-S6). Raltitrexed requires only a 15-min intravenous infusion for its administration, which improves patient compliance compared to oral medication problems, such as misuse, missed doses or multiple doses. In addition, due to its safety profile, some patients can complete their treatment on the day ward, thereby improving their quality of life. An advantage of the present study was its prospective design, over a wide range of Chinese regions that included patients aged from 20 years to 80 years regardless of RAS genotype and thus, the results are likely to be representative of the overall Chinese population.
In summary, exchanging 5-FU and oxaliplatin with SALIRI after first-line chemotherapy led to favorable mPFS and mOS, especially when combined with targeted drugs for the treatment of mCRC, which may solve the problem of repeated use resistance to 5-FU analogs and thus improve therapeutic outcomes.
Conceptualization: Shuqui Qin and Jin Li. Formal analysis: All authors. Investigation: All authors. Writing—original draft: Shuqui Qin and Jin Li. Writing—review & editing: All authors. Manuscript approval: All authors. Supervision: Jin Li. Project administration: Jin Li.
The authors declare no conflict of interest.
None.
The trial was in accordance with the Helsinki Declaration and was approved by the ethics committees of Tongji University Shanghai East Hospital (approval number: 2018-Research Review No. 12) and Bayi Hospital Nanjing Chinese Medicine University (approval number: 81YY-ZLLL-17-32). All patients signed informed consent forms. This study was registered with the Chinese Clinical Trial Registry (registration number: ChiCTR1800016185).
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
