Sining Xie, Federica Galimberti, Elena Olmastroni, Alberico L. Catapano, Manuela Casula
{"title":"在他汀类药物治疗中添加依折麦布、贝美多酸或秋水仙碱对 C 反应蛋白水平的影响:网络荟萃分析","authors":"Sining Xie, Federica Galimberti, Elena Olmastroni, Alberico L. Catapano, Manuela Casula","doi":"10.1111/joim.13824","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of morbidity and mortality worldwide. Although several therapeutic options are available to reduce LDL-cholesterol (LDL-C), many patients continue to experience major cardiovascular (CV) events. In ASCVD, inflammation plays a critical role, contributing significantly to residual CV risk [<span>1</span>]. Several anti-inflammatory therapies have been evaluated to reduce CV risk, and recently, the U.S. Food and Drug Administration approved the use of low-dose colchicine to reduce the risk of myocardial infarction (MI), stroke, coronary revascularization, or CV death in adult patients with established ASCVD or multiple CV risk factors [<span>2, 3</span>]. Meta-analyses have shown that low-dose colchicine (0.5–1.0 mg) can lead to a reduction in C-reactive protein (CRP) levels by −0.36 mg/L (95%CI, −0.51 to −0.20) in patients with coronary artery disease [<span>4, 5</span>], and by −0.66 mg/L (95%CI, −0.98 to −0.35) in patients with acute MI [<span>6</span>], which translates into a 35% and 44% reduction in major CV events, respectively. Nevertheless, some studies have suggested an anti-inflammatory effect with some lipid-lowering therapies. In a recent meta-analysis involving 171,668 subjects from 53 randomized control trials (RCTs), we demonstrated a reduction in serum CRP concentration with statins (−0.65 mg/L [95%CI, −0.87 to −0.43]), bempedoic acid (−0.43 mg/L [95%CI, −0.67 to −0.20]), and ezetimibe (−0.28 mg/L [95%CI, −0.48 to −0.08]), which was independent of LDL-C changes [<span>7</span>].</p><p>Given the growing interest in targeting inflammation to further reduce CV risk and the recent inclusion of colchicine among CV preventive therapies [<span>8</span>], it appears of interest to compare the effect of available therapies on plasma CRP levels. Therefore, we sought to quantify the additional effect of adding colchicine to statins on CRP levels and to compare the effect of bempedoic acid, ezetimibe, or colchicine added to background statin treatment.</p><p>Because no trial directly compares the impact on CRP levels of colchicine versus lipid-lowering therapies, we performed a network meta-analysis according to the PRISMA guidelines. PubMed, Web of Science, EMBASE, Cochrane Library, and ClinicalTrial.gov were searched from inception to November 2023. Inclusion criteria were as follows: (1) RCTs in human, parallel design, phase II, III, or IV; (2) English language; (3) using ezetimibe, bempedoic acid, or colchicine as interventions on top of statin treatment (defined as more than 80% patients treated with statins at baseline); (4) reporting the effect on CRP levels; (5) with an intervention duration of more than 3 weeks.</p><p>Pooled estimates were assessed by both fixed-effect and random-effects models within a Bayesian hierarchical setting, assuming equal heterogeneity across all comparisons. When significant heterogeneity was detected (as determined by <i>t</i><sup>2</sup> and <i>I</i><sup>2</sup> statistics, <i>p</i> < 0.05), the results from the random-effects model were presented. We evaluated individual studies with the Cochrane risk of bias (RoB) tool [<span>9</span>]. Sensitivity analysis was performed by excluding trials with a high risk in the RoB evaluation. All the analyses were conducted by <i>gemtc</i> package in R (version 4.3.2). Additional information is provided in the Supporting Information section.</p><p>A total of 22,287 subjects from 30 RCTs (Table S1; median follow-up: 4.5 months) were included (22 RCTs for ezetimibe [18,386 subjects], 3 RCTs for bempedoic acid [2961 subjects], and 5 RCTs for colchicine [940 subjects]). Pairwise meta-analysis indicated that adding colchicine to statin reduced CRP levels by −0.75 mg/L (95% CI, −0.88 to −0.61) (Fig. 1a) compared to statin alone. In the network meta-analysis, the addition of colchicine on statin treatment showed no significant differences in the direct comparison to the add-on of ezetimibe (−0.22 mg/L [95% CI, −0.69 to 0.30]) or bempedoic acid (−0.44 mg/L [95% CI, −1.05 to 0.23]) (Fig. 1b, Figure S1). Bempedoic acid and ezetimibe, added to statin therapy, were not significantly different at reducing CRP levels (−0.22 mg/L [95% CI, −0.72 to 0.29]) (Fig. 1b). The results from the analysis comparing the effect on relative CRP changes (Figure S2) and the sensitivity analysis removing trials with high RoB (Table S2, Figures S3 and S4) were consistent.</p><p>In summary, our analysis suggests that the anti-inflammatory effect of ezetimibe, bempedoic acid, or colchicine on top of statin treatment appears to be comparable in the short term and further raises the question about which patients colchicine will benefit the most. In general, our data suggest that a patient not at goal for LDL-C with statin treatment and therefore eligible for a combination of lipid-lowering therapies will achieve benefits by the addition of ezetimibe or bempedoic acid in terms of CRP reduction comparable to that achieved with colchicine. Notably, although CRP has been consistently associated with CV risk, the causal nature of the association has not been demonstrated [<span>10</span>]. Furthermore, CRP may not capture all aspects of chronic inflammatory processes. Further research is warranted to explore the comparative medium- to long-term impact of these drugs on overall systemic inflammation.</p><p>Sining Xie and Manuela Casula made the contributions to the concept and design. Sining Xie and Federica Galimberti were responsible for the acquisition, analysis, and interpretation of data. Sining Xie and Elena Olmastroni did the statistical analysis. Sining Xie and Manuela Casula prepared the draft of the manuscript. All authors contributed to the critical revision of the manuscript. Alberico L. Catapano provided overall supervision of the study.</p><p>SX, FG, EO, and MC report no disclosures.</p><p>No funding was received for this project. The work of ALC, MC, and FG is supported in part by the grant Ricerca Corrente from the Italian Ministry of Health to IRCCS MultiMedica. ALC received research funding and/or honoraria for advisory boards, consultancy, or speaker bureaus from Amarin, Amgen, Amryt, AstraZeneca, Daiichi Sankyo, Esperion, Ionis Pharmaceuticals, Medscape, Menarini, Merck, Novartis, Peer Voice, Pfizer, Recordati, Regeneron, Sandoz, Sanofi, The Corpus, Ultragenyx, and Viatris.</p>","PeriodicalId":196,"journal":{"name":"Journal of Internal Medicine","volume":"296 3","pages":"302-305"},"PeriodicalIF":9.2000,"publicationDate":"2024-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.13824","citationCount":"0","resultStr":"{\"title\":\"Effect on C-reactive protein levels of the addition of ezetimibe, bempedoic acid, or colchicine to statin treatment: A network meta-analysis\",\"authors\":\"Sining Xie, Federica Galimberti, Elena Olmastroni, Alberico L. Catapano, Manuela Casula\",\"doi\":\"10.1111/joim.13824\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Dear Editor,</p><p>Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of morbidity and mortality worldwide. Although several therapeutic options are available to reduce LDL-cholesterol (LDL-C), many patients continue to experience major cardiovascular (CV) events. In ASCVD, inflammation plays a critical role, contributing significantly to residual CV risk [<span>1</span>]. Several anti-inflammatory therapies have been evaluated to reduce CV risk, and recently, the U.S. Food and Drug Administration approved the use of low-dose colchicine to reduce the risk of myocardial infarction (MI), stroke, coronary revascularization, or CV death in adult patients with established ASCVD or multiple CV risk factors [<span>2, 3</span>]. Meta-analyses have shown that low-dose colchicine (0.5–1.0 mg) can lead to a reduction in C-reactive protein (CRP) levels by −0.36 mg/L (95%CI, −0.51 to −0.20) in patients with coronary artery disease [<span>4, 5</span>], and by −0.66 mg/L (95%CI, −0.98 to −0.35) in patients with acute MI [<span>6</span>], which translates into a 35% and 44% reduction in major CV events, respectively. Nevertheless, some studies have suggested an anti-inflammatory effect with some lipid-lowering therapies. In a recent meta-analysis involving 171,668 subjects from 53 randomized control trials (RCTs), we demonstrated a reduction in serum CRP concentration with statins (−0.65 mg/L [95%CI, −0.87 to −0.43]), bempedoic acid (−0.43 mg/L [95%CI, −0.67 to −0.20]), and ezetimibe (−0.28 mg/L [95%CI, −0.48 to −0.08]), which was independent of LDL-C changes [<span>7</span>].</p><p>Given the growing interest in targeting inflammation to further reduce CV risk and the recent inclusion of colchicine among CV preventive therapies [<span>8</span>], it appears of interest to compare the effect of available therapies on plasma CRP levels. Therefore, we sought to quantify the additional effect of adding colchicine to statins on CRP levels and to compare the effect of bempedoic acid, ezetimibe, or colchicine added to background statin treatment.</p><p>Because no trial directly compares the impact on CRP levels of colchicine versus lipid-lowering therapies, we performed a network meta-analysis according to the PRISMA guidelines. PubMed, Web of Science, EMBASE, Cochrane Library, and ClinicalTrial.gov were searched from inception to November 2023. Inclusion criteria were as follows: (1) RCTs in human, parallel design, phase II, III, or IV; (2) English language; (3) using ezetimibe, bempedoic acid, or colchicine as interventions on top of statin treatment (defined as more than 80% patients treated with statins at baseline); (4) reporting the effect on CRP levels; (5) with an intervention duration of more than 3 weeks.</p><p>Pooled estimates were assessed by both fixed-effect and random-effects models within a Bayesian hierarchical setting, assuming equal heterogeneity across all comparisons. When significant heterogeneity was detected (as determined by <i>t</i><sup>2</sup> and <i>I</i><sup>2</sup> statistics, <i>p</i> < 0.05), the results from the random-effects model were presented. We evaluated individual studies with the Cochrane risk of bias (RoB) tool [<span>9</span>]. Sensitivity analysis was performed by excluding trials with a high risk in the RoB evaluation. All the analyses were conducted by <i>gemtc</i> package in R (version 4.3.2). Additional information is provided in the Supporting Information section.</p><p>A total of 22,287 subjects from 30 RCTs (Table S1; median follow-up: 4.5 months) were included (22 RCTs for ezetimibe [18,386 subjects], 3 RCTs for bempedoic acid [2961 subjects], and 5 RCTs for colchicine [940 subjects]). Pairwise meta-analysis indicated that adding colchicine to statin reduced CRP levels by −0.75 mg/L (95% CI, −0.88 to −0.61) (Fig. 1a) compared to statin alone. In the network meta-analysis, the addition of colchicine on statin treatment showed no significant differences in the direct comparison to the add-on of ezetimibe (−0.22 mg/L [95% CI, −0.69 to 0.30]) or bempedoic acid (−0.44 mg/L [95% CI, −1.05 to 0.23]) (Fig. 1b, Figure S1). Bempedoic acid and ezetimibe, added to statin therapy, were not significantly different at reducing CRP levels (−0.22 mg/L [95% CI, −0.72 to 0.29]) (Fig. 1b). The results from the analysis comparing the effect on relative CRP changes (Figure S2) and the sensitivity analysis removing trials with high RoB (Table S2, Figures S3 and S4) were consistent.</p><p>In summary, our analysis suggests that the anti-inflammatory effect of ezetimibe, bempedoic acid, or colchicine on top of statin treatment appears to be comparable in the short term and further raises the question about which patients colchicine will benefit the most. In general, our data suggest that a patient not at goal for LDL-C with statin treatment and therefore eligible for a combination of lipid-lowering therapies will achieve benefits by the addition of ezetimibe or bempedoic acid in terms of CRP reduction comparable to that achieved with colchicine. Notably, although CRP has been consistently associated with CV risk, the causal nature of the association has not been demonstrated [<span>10</span>]. Furthermore, CRP may not capture all aspects of chronic inflammatory processes. Further research is warranted to explore the comparative medium- to long-term impact of these drugs on overall systemic inflammation.</p><p>Sining Xie and Manuela Casula made the contributions to the concept and design. Sining Xie and Federica Galimberti were responsible for the acquisition, analysis, and interpretation of data. Sining Xie and Elena Olmastroni did the statistical analysis. Sining Xie and Manuela Casula prepared the draft of the manuscript. All authors contributed to the critical revision of the manuscript. Alberico L. Catapano provided overall supervision of the study.</p><p>SX, FG, EO, and MC report no disclosures.</p><p>No funding was received for this project. The work of ALC, MC, and FG is supported in part by the grant Ricerca Corrente from the Italian Ministry of Health to IRCCS MultiMedica. ALC received research funding and/or honoraria for advisory boards, consultancy, or speaker bureaus from Amarin, Amgen, Amryt, AstraZeneca, Daiichi Sankyo, Esperion, Ionis Pharmaceuticals, Medscape, Menarini, Merck, Novartis, Peer Voice, Pfizer, Recordati, Regeneron, Sandoz, Sanofi, The Corpus, Ultragenyx, and Viatris.</p>\",\"PeriodicalId\":196,\"journal\":{\"name\":\"Journal of Internal Medicine\",\"volume\":\"296 3\",\"pages\":\"302-305\"},\"PeriodicalIF\":9.2000,\"publicationDate\":\"2024-07-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.13824\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Internal Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/joim.13824\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/joim.13824","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Effect on C-reactive protein levels of the addition of ezetimibe, bempedoic acid, or colchicine to statin treatment: A network meta-analysis
Dear Editor,
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of morbidity and mortality worldwide. Although several therapeutic options are available to reduce LDL-cholesterol (LDL-C), many patients continue to experience major cardiovascular (CV) events. In ASCVD, inflammation plays a critical role, contributing significantly to residual CV risk [1]. Several anti-inflammatory therapies have been evaluated to reduce CV risk, and recently, the U.S. Food and Drug Administration approved the use of low-dose colchicine to reduce the risk of myocardial infarction (MI), stroke, coronary revascularization, or CV death in adult patients with established ASCVD or multiple CV risk factors [2, 3]. Meta-analyses have shown that low-dose colchicine (0.5–1.0 mg) can lead to a reduction in C-reactive protein (CRP) levels by −0.36 mg/L (95%CI, −0.51 to −0.20) in patients with coronary artery disease [4, 5], and by −0.66 mg/L (95%CI, −0.98 to −0.35) in patients with acute MI [6], which translates into a 35% and 44% reduction in major CV events, respectively. Nevertheless, some studies have suggested an anti-inflammatory effect with some lipid-lowering therapies. In a recent meta-analysis involving 171,668 subjects from 53 randomized control trials (RCTs), we demonstrated a reduction in serum CRP concentration with statins (−0.65 mg/L [95%CI, −0.87 to −0.43]), bempedoic acid (−0.43 mg/L [95%CI, −0.67 to −0.20]), and ezetimibe (−0.28 mg/L [95%CI, −0.48 to −0.08]), which was independent of LDL-C changes [7].
Given the growing interest in targeting inflammation to further reduce CV risk and the recent inclusion of colchicine among CV preventive therapies [8], it appears of interest to compare the effect of available therapies on plasma CRP levels. Therefore, we sought to quantify the additional effect of adding colchicine to statins on CRP levels and to compare the effect of bempedoic acid, ezetimibe, or colchicine added to background statin treatment.
Because no trial directly compares the impact on CRP levels of colchicine versus lipid-lowering therapies, we performed a network meta-analysis according to the PRISMA guidelines. PubMed, Web of Science, EMBASE, Cochrane Library, and ClinicalTrial.gov were searched from inception to November 2023. Inclusion criteria were as follows: (1) RCTs in human, parallel design, phase II, III, or IV; (2) English language; (3) using ezetimibe, bempedoic acid, or colchicine as interventions on top of statin treatment (defined as more than 80% patients treated with statins at baseline); (4) reporting the effect on CRP levels; (5) with an intervention duration of more than 3 weeks.
Pooled estimates were assessed by both fixed-effect and random-effects models within a Bayesian hierarchical setting, assuming equal heterogeneity across all comparisons. When significant heterogeneity was detected (as determined by t2 and I2 statistics, p < 0.05), the results from the random-effects model were presented. We evaluated individual studies with the Cochrane risk of bias (RoB) tool [9]. Sensitivity analysis was performed by excluding trials with a high risk in the RoB evaluation. All the analyses were conducted by gemtc package in R (version 4.3.2). Additional information is provided in the Supporting Information section.
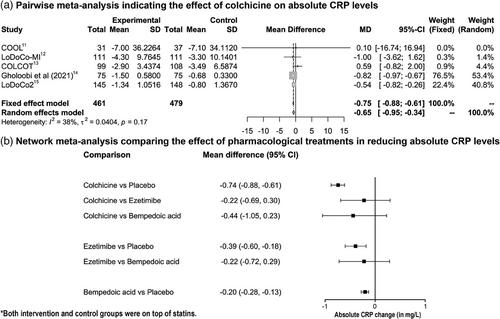
A total of 22,287 subjects from 30 RCTs (Table S1; median follow-up: 4.5 months) were included (22 RCTs for ezetimibe [18,386 subjects], 3 RCTs for bempedoic acid [2961 subjects], and 5 RCTs for colchicine [940 subjects]). Pairwise meta-analysis indicated that adding colchicine to statin reduced CRP levels by −0.75 mg/L (95% CI, −0.88 to −0.61) (Fig. 1a) compared to statin alone. In the network meta-analysis, the addition of colchicine on statin treatment showed no significant differences in the direct comparison to the add-on of ezetimibe (−0.22 mg/L [95% CI, −0.69 to 0.30]) or bempedoic acid (−0.44 mg/L [95% CI, −1.05 to 0.23]) (Fig. 1b, Figure S1). Bempedoic acid and ezetimibe, added to statin therapy, were not significantly different at reducing CRP levels (−0.22 mg/L [95% CI, −0.72 to 0.29]) (Fig. 1b). The results from the analysis comparing the effect on relative CRP changes (Figure S2) and the sensitivity analysis removing trials with high RoB (Table S2, Figures S3 and S4) were consistent.
In summary, our analysis suggests that the anti-inflammatory effect of ezetimibe, bempedoic acid, or colchicine on top of statin treatment appears to be comparable in the short term and further raises the question about which patients colchicine will benefit the most. In general, our data suggest that a patient not at goal for LDL-C with statin treatment and therefore eligible for a combination of lipid-lowering therapies will achieve benefits by the addition of ezetimibe or bempedoic acid in terms of CRP reduction comparable to that achieved with colchicine. Notably, although CRP has been consistently associated with CV risk, the causal nature of the association has not been demonstrated [10]. Furthermore, CRP may not capture all aspects of chronic inflammatory processes. Further research is warranted to explore the comparative medium- to long-term impact of these drugs on overall systemic inflammation.
Sining Xie and Manuela Casula made the contributions to the concept and design. Sining Xie and Federica Galimberti were responsible for the acquisition, analysis, and interpretation of data. Sining Xie and Elena Olmastroni did the statistical analysis. Sining Xie and Manuela Casula prepared the draft of the manuscript. All authors contributed to the critical revision of the manuscript. Alberico L. Catapano provided overall supervision of the study.
SX, FG, EO, and MC report no disclosures.
No funding was received for this project. The work of ALC, MC, and FG is supported in part by the grant Ricerca Corrente from the Italian Ministry of Health to IRCCS MultiMedica. ALC received research funding and/or honoraria for advisory boards, consultancy, or speaker bureaus from Amarin, Amgen, Amryt, AstraZeneca, Daiichi Sankyo, Esperion, Ionis Pharmaceuticals, Medscape, Menarini, Merck, Novartis, Peer Voice, Pfizer, Recordati, Regeneron, Sandoz, Sanofi, The Corpus, Ultragenyx, and Viatris.
期刊介绍:
JIM – The Journal of Internal Medicine, in continuous publication since 1863, is an international, peer-reviewed scientific journal. It publishes original work in clinical science, spanning from bench to bedside, encompassing a wide range of internal medicine and its subspecialties. JIM showcases original articles, reviews, brief reports, and research letters in the field of internal medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
