Poornima Vinod, Vinod Krishnappa, William Rathell, Saira Amir, Subrina Sundil, Godwin Dogbey, Hiten Patel, William Herzog
{"title":"使用阿司匹林对 COVID-19 住院患者不良后果的影响","authors":"Poornima Vinod, Vinod Krishnappa, William Rathell, Saira Amir, Subrina Sundil, Godwin Dogbey, Hiten Patel, William Herzog","doi":"10.14740/cr1645","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronavirus disease 2019 (COVID-19) triggers multiple components of the immune system and causes inflammation of endothelial walls across vascular beds, resulting in respiratory failure, arterial and venous thrombosis, myocardial injury, and multi-organ failure leading to death. Early in the COVID-19 pandemic, aspirin was suggested for the treatment of symptomatic individuals, given its analgesic, antipyretic, anti-inflammatory, anti-thrombotic, and antiviral effects. This study aimed to evaluate the association of aspirin use with various clinical outcomes in patients hospitalized for COVID-19.</p><p><strong>Methods: </strong>This was a retrospective study involving patients aged ≥ 18 years and hospitalized for COVID-19 from March 2020 to October 2020. Primary outcomes were acute cardiovascular events (ST elevation myocardial infarction (STEMI), type 1 non-ST elevation myocardial infarction (NSTEMI), acute congestive heart failure (CHF), and acute stroke) and death. Secondary outcomes were respiratory failure, need for mechanical ventilation, and acute deep vein thrombosis (DVT)/pulmonary embolism (PE).</p><p><strong>Results: </strong>Of 376 patients hospitalized for COVID-19, 128 were taking aspirin. Significant proportions of native Americans were hospitalized for COVID-19 in both aspirin (22.7%) and non-aspirin (24.6%) groups. Between aspirin and non-aspirin groups, no significant differences were found with regard to mechanical ventilator support (21.1% vs. 15.3%, P = 0.16), acute cardiovascular events (7.8% vs. 5.2%, P = 0.32), acute DVT/PE (3.9% vs. 5.2%, P = 0.9), readmission rate (13.3% vs. 12.9%, P = 0.91) and mortality (23.4% vs. 20.2%, P = 0.5); however, the median duration of mechanical ventilation was significantly shorter (7 vs. 9 days, P = 0.04) and median length of hospitalization was significantly longer (5.5 vs. 4 days, P = 0.01) in aspirin group compared to non-aspirin group.</p><p><strong>Conclusion: </strong>No significant differences were found in acute cardiovascular events, acute DVT/PE, mechanical ventilator support, and mortality rate between hospitalized COVID-19 patients who were taking aspirin compared to those not taking aspirin. However, larger studies are required to confirm our findings.</p>","PeriodicalId":9424,"journal":{"name":"Cardiology Research","volume":"15 3","pages":"179-188"},"PeriodicalIF":1.4000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11236346/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of Aspirin Use on the Adverse Outcomes in Patients Hospitalized for COVID-19.\",\"authors\":\"Poornima Vinod, Vinod Krishnappa, William Rathell, Saira Amir, Subrina Sundil, Godwin Dogbey, Hiten Patel, William Herzog\",\"doi\":\"10.14740/cr1645\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Coronavirus disease 2019 (COVID-19) triggers multiple components of the immune system and causes inflammation of endothelial walls across vascular beds, resulting in respiratory failure, arterial and venous thrombosis, myocardial injury, and multi-organ failure leading to death. Early in the COVID-19 pandemic, aspirin was suggested for the treatment of symptomatic individuals, given its analgesic, antipyretic, anti-inflammatory, anti-thrombotic, and antiviral effects. This study aimed to evaluate the association of aspirin use with various clinical outcomes in patients hospitalized for COVID-19.</p><p><strong>Methods: </strong>This was a retrospective study involving patients aged ≥ 18 years and hospitalized for COVID-19 from March 2020 to October 2020. Primary outcomes were acute cardiovascular events (ST elevation myocardial infarction (STEMI), type 1 non-ST elevation myocardial infarction (NSTEMI), acute congestive heart failure (CHF), and acute stroke) and death. Secondary outcomes were respiratory failure, need for mechanical ventilation, and acute deep vein thrombosis (DVT)/pulmonary embolism (PE).</p><p><strong>Results: </strong>Of 376 patients hospitalized for COVID-19, 128 were taking aspirin. Significant proportions of native Americans were hospitalized for COVID-19 in both aspirin (22.7%) and non-aspirin (24.6%) groups. Between aspirin and non-aspirin groups, no significant differences were found with regard to mechanical ventilator support (21.1% vs. 15.3%, P = 0.16), acute cardiovascular events (7.8% vs. 5.2%, P = 0.32), acute DVT/PE (3.9% vs. 5.2%, P = 0.9), readmission rate (13.3% vs. 12.9%, P = 0.91) and mortality (23.4% vs. 20.2%, P = 0.5); however, the median duration of mechanical ventilation was significantly shorter (7 vs. 9 days, P = 0.04) and median length of hospitalization was significantly longer (5.5 vs. 4 days, P = 0.01) in aspirin group compared to non-aspirin group.</p><p><strong>Conclusion: </strong>No significant differences were found in acute cardiovascular events, acute DVT/PE, mechanical ventilator support, and mortality rate between hospitalized COVID-19 patients who were taking aspirin compared to those not taking aspirin. However, larger studies are required to confirm our findings.</p>\",\"PeriodicalId\":9424,\"journal\":{\"name\":\"Cardiology Research\",\"volume\":\"15 3\",\"pages\":\"179-188\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11236346/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/cr1645\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/cr1645","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:2019 年冠状病毒病(COVID-19)会引发免疫系统的多种成分,并导致血管床内皮壁发炎,导致呼吸衰竭、动静脉血栓形成、心肌损伤和多器官衰竭,最终导致死亡。在 COVID-19 大流行的早期,由于阿司匹林具有镇痛、解热、消炎、抗血栓和抗病毒的作用,因此被建议用于治疗有症状的患者。本研究旨在评估因 COVID-19 而住院的患者使用阿司匹林与各种临床结果之间的关系:这是一项回顾性研究,涉及 2020 年 3 月至 2020 年 10 月期间因 COVID-19 住院且年龄≥ 18 岁的患者。主要结果为急性心血管事件(ST段抬高型心肌梗死(STEMI)、1型非ST段抬高型心肌梗死(NSTEMI)、急性充血性心力衰竭(CHF)和急性卒中)和死亡。次要结果为呼吸衰竭、机械通气需求和急性深静脉血栓(DVT)/肺栓塞(PE):在376名因COVID-19住院的患者中,有128人服用阿司匹林。在阿司匹林组(22.7%)和非阿司匹林组(24.6%)中,因 COVID-19 住院的美国本地人比例都很高。阿司匹林组和非阿司匹林组在机械呼吸机支持(21.1% vs. 15.3%,P = 0.16)、急性心血管事件(7.8% vs. 5.2%,P = 0.32)、急性深静脉血栓/PE(3.9% vs. 5.2%,P = 0.9)、再入院率(13.3% vs. 12.9%,P = 0.91)和死亡率(23.4% vs. 20.2%,P = 0.5);然而,与非阿司匹林组相比,阿司匹林组机械通气的中位持续时间显著缩短(7 vs. 9天,P = 0.04),中位住院时间显著延长(5.5 vs. 4天,P = 0.01):结论:与未服用阿司匹林的患者相比,服用阿司匹林的 COVID-19 住院患者在急性心血管事件、急性深静脉血栓/动脉粥样硬化、机械呼吸机支持和死亡率方面无明显差异。不过,还需要更大规模的研究来证实我们的发现。
Effect of Aspirin Use on the Adverse Outcomes in Patients Hospitalized for COVID-19.
Background: Coronavirus disease 2019 (COVID-19) triggers multiple components of the immune system and causes inflammation of endothelial walls across vascular beds, resulting in respiratory failure, arterial and venous thrombosis, myocardial injury, and multi-organ failure leading to death. Early in the COVID-19 pandemic, aspirin was suggested for the treatment of symptomatic individuals, given its analgesic, antipyretic, anti-inflammatory, anti-thrombotic, and antiviral effects. This study aimed to evaluate the association of aspirin use with various clinical outcomes in patients hospitalized for COVID-19.
Methods: This was a retrospective study involving patients aged ≥ 18 years and hospitalized for COVID-19 from March 2020 to October 2020. Primary outcomes were acute cardiovascular events (ST elevation myocardial infarction (STEMI), type 1 non-ST elevation myocardial infarction (NSTEMI), acute congestive heart failure (CHF), and acute stroke) and death. Secondary outcomes were respiratory failure, need for mechanical ventilation, and acute deep vein thrombosis (DVT)/pulmonary embolism (PE).
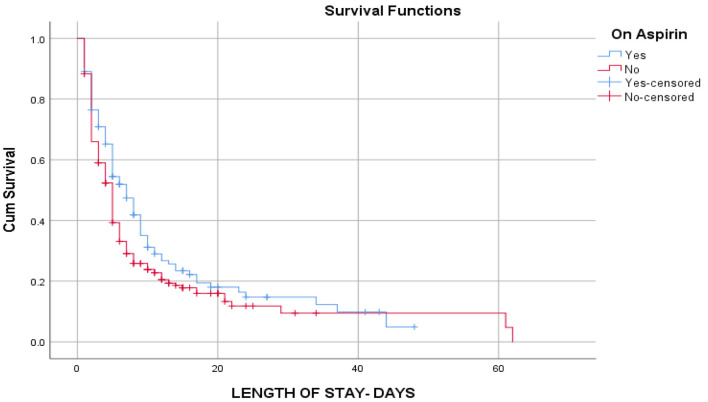
Results: Of 376 patients hospitalized for COVID-19, 128 were taking aspirin. Significant proportions of native Americans were hospitalized for COVID-19 in both aspirin (22.7%) and non-aspirin (24.6%) groups. Between aspirin and non-aspirin groups, no significant differences were found with regard to mechanical ventilator support (21.1% vs. 15.3%, P = 0.16), acute cardiovascular events (7.8% vs. 5.2%, P = 0.32), acute DVT/PE (3.9% vs. 5.2%, P = 0.9), readmission rate (13.3% vs. 12.9%, P = 0.91) and mortality (23.4% vs. 20.2%, P = 0.5); however, the median duration of mechanical ventilation was significantly shorter (7 vs. 9 days, P = 0.04) and median length of hospitalization was significantly longer (5.5 vs. 4 days, P = 0.01) in aspirin group compared to non-aspirin group.
Conclusion: No significant differences were found in acute cardiovascular events, acute DVT/PE, mechanical ventilator support, and mortality rate between hospitalized COVID-19 patients who were taking aspirin compared to those not taking aspirin. However, larger studies are required to confirm our findings.
期刊介绍:
Cardiology Research is an open access, peer-reviewed, international journal. All submissions relating to basic research and clinical practice of cardiology and cardiovascular medicine are in this journal''s scope. This journal focuses on publishing original research and observations in all cardiovascular medicine aspects. Manuscript types include original article, review, case report, short communication, book review, letter to the editor.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
