{"title":"需要与肝外胆管癌鉴别的胆管周围腺体增生:病例报告。","authors":"Kazuhiro Takami, Kuniharu Yamamoto, Hiroto Sakurai, Yoshihiro Sato, Noriko Kondo, Toru Nakano, Shingo Tsujinaka, Akinobu Koiwai, Morihisa Hirota, Keigo Murakami, Kazuhiro Murakami, Chikashi Shibata, Yu Katayose","doi":"10.1159/000538491","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The peribiliary gland is an accessory bile duct gland. Hyperplasia of these tissues may lead to elevation of the mucosa in the bile ducts and bile duct stenosis. We herein report a case of peribiliary gland hyperplasia that required preoperative differentiation from bile duct cancer, with a discussion of the literature.</p><p><strong>Case presentation: </strong>The patient had an adenomatous lesion in the ascending colon that was difficult to treat endoscopically; therefore, surgery was planned. Preoperative abdominal ultrasonography revealed a bile duct tumor, and endoscopic ultrasonography revealed a mass lesion around the confluence of the cystic duct. Computed tomography revealed localized wall thickening in the middle bile duct, and the upstream bile ducts were slightly dilated. In addition, continuous thickening of the bile duct wall from the gallbladder to the confluence of the cystic duct was observed. No distant metastases, such as liver metastases, or nearby enlarged lymph nodes were observed. Endoscopic retrograde cholangiopancreatography and magnetic resonance cholangiopancreatography revealed a papillary-like elevated lesion in the bile duct near the confluence of the cystic duct, and a biopsy and bile cytology from the same area showed no malignant findings. As a result, the possibility that the patient had gallbladder or bile duct cancer could not be ruled out; therefore, a policy of surgery together with the ascending colon tumor was decided after receiving sufficient informed consent. During surgery, the patient underwent extrahepatic bile duct resection, reconstruction of the biliary tract using the Roux-en-Y method, and right hemicolectomy. Both duodenal and hilar bile duct transects were subjected to a fast frozen section analysis during surgery, and the results were negative for cancer. A histopathological examination of the resected specimen revealed no malignant findings in the bile duct lesions, and a diagnosis of peribiliary gland hyperplasia with chronic inflammatory cell infiltration and fibrosis of the extrahepatic bile duct wall was made.</p><p><strong>Conclusions: </strong>We encountered a case of peribiliary gland hyperplasia that was difficult to distinguish from bile duct cancer.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"18 1","pages":"279-285"},"PeriodicalIF":0.6000,"publicationDate":"2024-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11249448/pdf/","citationCount":"0","resultStr":"{\"title\":\"Peribiliary Gland Hyperplasia That Required Differentiation from Extrahepatic Bile Duct Cancer: A Case Report.\",\"authors\":\"Kazuhiro Takami, Kuniharu Yamamoto, Hiroto Sakurai, Yoshihiro Sato, Noriko Kondo, Toru Nakano, Shingo Tsujinaka, Akinobu Koiwai, Morihisa Hirota, Keigo Murakami, Kazuhiro Murakami, Chikashi Shibata, Yu Katayose\",\"doi\":\"10.1159/000538491\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The peribiliary gland is an accessory bile duct gland. Hyperplasia of these tissues may lead to elevation of the mucosa in the bile ducts and bile duct stenosis. We herein report a case of peribiliary gland hyperplasia that required preoperative differentiation from bile duct cancer, with a discussion of the literature.</p><p><strong>Case presentation: </strong>The patient had an adenomatous lesion in the ascending colon that was difficult to treat endoscopically; therefore, surgery was planned. Preoperative abdominal ultrasonography revealed a bile duct tumor, and endoscopic ultrasonography revealed a mass lesion around the confluence of the cystic duct. Computed tomography revealed localized wall thickening in the middle bile duct, and the upstream bile ducts were slightly dilated. In addition, continuous thickening of the bile duct wall from the gallbladder to the confluence of the cystic duct was observed. No distant metastases, such as liver metastases, or nearby enlarged lymph nodes were observed. Endoscopic retrograde cholangiopancreatography and magnetic resonance cholangiopancreatography revealed a papillary-like elevated lesion in the bile duct near the confluence of the cystic duct, and a biopsy and bile cytology from the same area showed no malignant findings. As a result, the possibility that the patient had gallbladder or bile duct cancer could not be ruled out; therefore, a policy of surgery together with the ascending colon tumor was decided after receiving sufficient informed consent. During surgery, the patient underwent extrahepatic bile duct resection, reconstruction of the biliary tract using the Roux-en-Y method, and right hemicolectomy. Both duodenal and hilar bile duct transects were subjected to a fast frozen section analysis during surgery, and the results were negative for cancer. A histopathological examination of the resected specimen revealed no malignant findings in the bile duct lesions, and a diagnosis of peribiliary gland hyperplasia with chronic inflammatory cell infiltration and fibrosis of the extrahepatic bile duct wall was made.</p><p><strong>Conclusions: </strong>We encountered a case of peribiliary gland hyperplasia that was difficult to distinguish from bile duct cancer.</p>\",\"PeriodicalId\":9614,\"journal\":{\"name\":\"Case Reports in Gastroenterology\",\"volume\":\"18 1\",\"pages\":\"279-285\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2024-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11249448/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000538491\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000538491","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Peribiliary Gland Hyperplasia That Required Differentiation from Extrahepatic Bile Duct Cancer: A Case Report.
Introduction: The peribiliary gland is an accessory bile duct gland. Hyperplasia of these tissues may lead to elevation of the mucosa in the bile ducts and bile duct stenosis. We herein report a case of peribiliary gland hyperplasia that required preoperative differentiation from bile duct cancer, with a discussion of the literature.
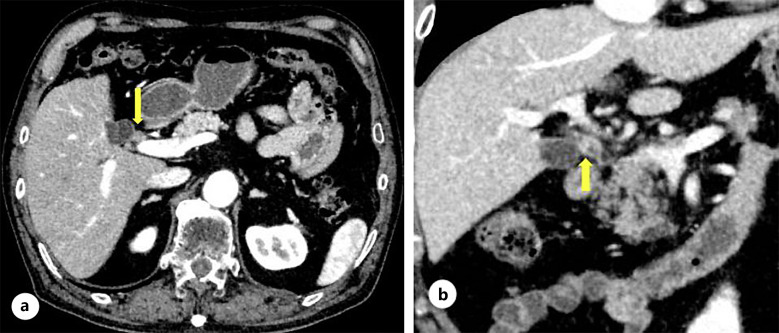
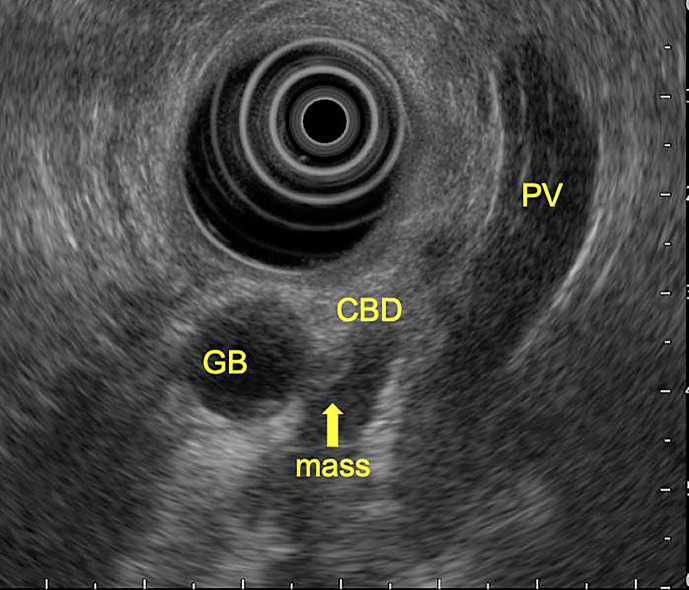
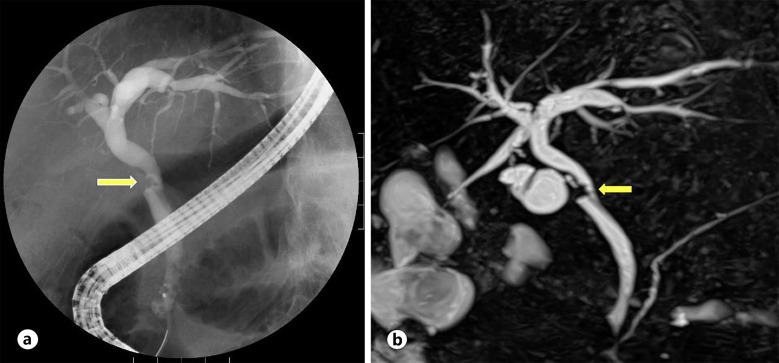
Case presentation: The patient had an adenomatous lesion in the ascending colon that was difficult to treat endoscopically; therefore, surgery was planned. Preoperative abdominal ultrasonography revealed a bile duct tumor, and endoscopic ultrasonography revealed a mass lesion around the confluence of the cystic duct. Computed tomography revealed localized wall thickening in the middle bile duct, and the upstream bile ducts were slightly dilated. In addition, continuous thickening of the bile duct wall from the gallbladder to the confluence of the cystic duct was observed. No distant metastases, such as liver metastases, or nearby enlarged lymph nodes were observed. Endoscopic retrograde cholangiopancreatography and magnetic resonance cholangiopancreatography revealed a papillary-like elevated lesion in the bile duct near the confluence of the cystic duct, and a biopsy and bile cytology from the same area showed no malignant findings. As a result, the possibility that the patient had gallbladder or bile duct cancer could not be ruled out; therefore, a policy of surgery together with the ascending colon tumor was decided after receiving sufficient informed consent. During surgery, the patient underwent extrahepatic bile duct resection, reconstruction of the biliary tract using the Roux-en-Y method, and right hemicolectomy. Both duodenal and hilar bile duct transects were subjected to a fast frozen section analysis during surgery, and the results were negative for cancer. A histopathological examination of the resected specimen revealed no malignant findings in the bile duct lesions, and a diagnosis of peribiliary gland hyperplasia with chronic inflammatory cell infiltration and fibrosis of the extrahepatic bile duct wall was made.
Conclusions: We encountered a case of peribiliary gland hyperplasia that was difficult to distinguish from bile duct cancer.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
