{"title":"耐药性高血压:诊断、评估和治疗--泰国高血压学会临床共识声明。","authors":"Pairoj Chattranukulchai, Weranuj Roubsanthisuk, Sirisawat Kunanon, Praew Kotruchin, Bancha Satirapoj, Nattawut Wongpraparut, Sarat Sunthornyothin, Apichard Sukonthasarn","doi":"10.1038/s41440-024-01785-6","DOIUrl":null,"url":null,"abstract":"Resistant hypertension (RH) includes hypertensive patients with uncontrolled blood pressure (BP) while receiving ≥3 BP-lowering medications or with controlled BP while receiving ≥4 BP-lowering medications. The exact prevalence of RH is challenging to quantify. However, a reasonable estimate of true RH is around 5% of the hypertensive population. Patients with RH have higher cardiovascular risk as compared with hypertensive patients in general. Standardized office BP measurement, confirmation of medical adherence, search for drug- or substance-induced BP elevation, and ambulatory or home BP monitoring are mandatory to exclude pseudoresistance. Appropriate further investigations, guided by clinical data, should be pursued to exclude possible secondary causes of hypertension. The management of RH includes the intensification of lifestyle interventions and the modification of antihypertensive drug regimens. The essential aspects of lifestyle modification include sodium restriction, body weight control, regular exercise, and healthy sleep. Step-by-step adjustment of the BP-lowering drugs based on the available evidence is proposed. The suitable choice of diuretics according to patients’ renal function is presented. Sacubitril/valsartan can be carefully substituted for the prior renin-angiotensin system blockers, especially in those with heart failure with preserved ejection fraction. If BP remains uncontrolled, device therapy such as renal nerve denervation should be considered. Since device-based treatment is an invasive and costly procedure, it should be used only after careful and appropriate case selection. In real-world practice, the management of RH should be individualized depending on each patient’s characteristics.","PeriodicalId":13029,"journal":{"name":"Hypertension Research","volume":"47 9","pages":"2447-2455"},"PeriodicalIF":5.0000,"publicationDate":"2024-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.com/articles/s41440-024-01785-6.pdf","citationCount":"0","resultStr":"{\"title\":\"Resistant hypertension: diagnosis, evaluation, and treatment a clinical consensus statement from the Thai hypertension society\",\"authors\":\"Pairoj Chattranukulchai, Weranuj Roubsanthisuk, Sirisawat Kunanon, Praew Kotruchin, Bancha Satirapoj, Nattawut Wongpraparut, Sarat Sunthornyothin, Apichard Sukonthasarn\",\"doi\":\"10.1038/s41440-024-01785-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Resistant hypertension (RH) includes hypertensive patients with uncontrolled blood pressure (BP) while receiving ≥3 BP-lowering medications or with controlled BP while receiving ≥4 BP-lowering medications. The exact prevalence of RH is challenging to quantify. However, a reasonable estimate of true RH is around 5% of the hypertensive population. Patients with RH have higher cardiovascular risk as compared with hypertensive patients in general. Standardized office BP measurement, confirmation of medical adherence, search for drug- or substance-induced BP elevation, and ambulatory or home BP monitoring are mandatory to exclude pseudoresistance. Appropriate further investigations, guided by clinical data, should be pursued to exclude possible secondary causes of hypertension. The management of RH includes the intensification of lifestyle interventions and the modification of antihypertensive drug regimens. The essential aspects of lifestyle modification include sodium restriction, body weight control, regular exercise, and healthy sleep. Step-by-step adjustment of the BP-lowering drugs based on the available evidence is proposed. The suitable choice of diuretics according to patients’ renal function is presented. Sacubitril/valsartan can be carefully substituted for the prior renin-angiotensin system blockers, especially in those with heart failure with preserved ejection fraction. If BP remains uncontrolled, device therapy such as renal nerve denervation should be considered. Since device-based treatment is an invasive and costly procedure, it should be used only after careful and appropriate case selection. In real-world practice, the management of RH should be individualized depending on each patient’s characteristics.\",\"PeriodicalId\":13029,\"journal\":{\"name\":\"Hypertension Research\",\"volume\":\"47 9\",\"pages\":\"2447-2455\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-07-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.nature.com/articles/s41440-024-01785-6.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hypertension Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.nature.com/articles/s41440-024-01785-6\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hypertension Research","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41440-024-01785-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Resistant hypertension: diagnosis, evaluation, and treatment a clinical consensus statement from the Thai hypertension society
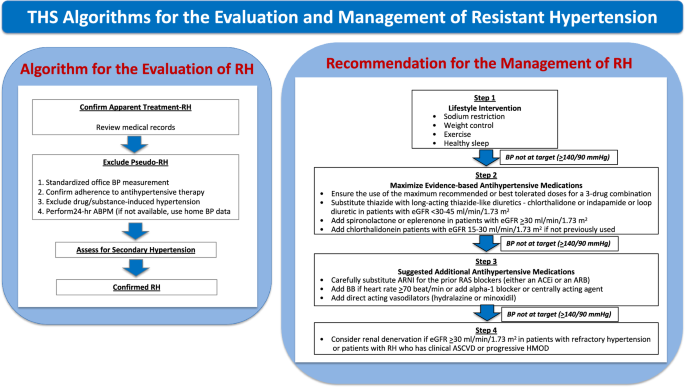
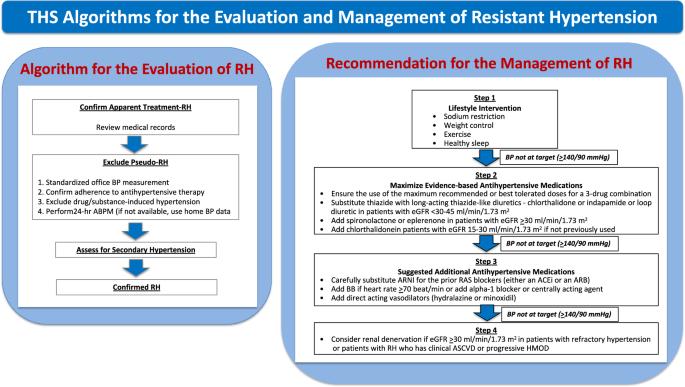
Resistant hypertension (RH) includes hypertensive patients with uncontrolled blood pressure (BP) while receiving ≥3 BP-lowering medications or with controlled BP while receiving ≥4 BP-lowering medications. The exact prevalence of RH is challenging to quantify. However, a reasonable estimate of true RH is around 5% of the hypertensive population. Patients with RH have higher cardiovascular risk as compared with hypertensive patients in general. Standardized office BP measurement, confirmation of medical adherence, search for drug- or substance-induced BP elevation, and ambulatory or home BP monitoring are mandatory to exclude pseudoresistance. Appropriate further investigations, guided by clinical data, should be pursued to exclude possible secondary causes of hypertension. The management of RH includes the intensification of lifestyle interventions and the modification of antihypertensive drug regimens. The essential aspects of lifestyle modification include sodium restriction, body weight control, regular exercise, and healthy sleep. Step-by-step adjustment of the BP-lowering drugs based on the available evidence is proposed. The suitable choice of diuretics according to patients’ renal function is presented. Sacubitril/valsartan can be carefully substituted for the prior renin-angiotensin system blockers, especially in those with heart failure with preserved ejection fraction. If BP remains uncontrolled, device therapy such as renal nerve denervation should be considered. Since device-based treatment is an invasive and costly procedure, it should be used only after careful and appropriate case selection. In real-world practice, the management of RH should be individualized depending on each patient’s characteristics.
期刊介绍:
Hypertension Research is the official publication of the Japanese Society of Hypertension. The journal publishes papers reporting original clinical and experimental research that contribute to the advancement of knowledge in the field of hypertension and related cardiovascular diseases. The journal publishes Review Articles, Articles, Correspondence and Comments.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
