Katelyn N. Rudzik, Kristine S. Schonder, Abhinav Humar, Heather J. Johnson
{"title":"活体肝移植后 180 天内尽早转用依维莫司。","authors":"Katelyn N. Rudzik, Kristine S. Schonder, Abhinav Humar, Heather J. Johnson","doi":"10.1111/ctr.15402","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Early conversion to Everolimus (EVR) post deceased donor liver transplant has been associated with improved renal function but increased rejection. Early EVR conversion has not been evaluated after living donor liver transplant (LDLT). A retrospective cohort study was conducted to compare the rate of rejection and renal function in patients converted to EVR early post-LDLT to patients on calcineurin inhibitors (CNIs).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a single center retrospective cohort study of adult LDLT recipients between January 2012 and July 2019. Patients converted to EVR within 180 days of transplant were compared to patients on CNIs. The primary endpoint was biopsy proven acute rejection (BPAR) at 24 months posttransplant. Key secondary endpoints included eGFR at 24 months, change in eGFR, adverse events, and all-cause mortality.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>From a total of 173 patients involved in the study: 58 were included in the EVR group and 115 in the CNI group. Median conversion to EVR was 26 days post-LDLT. At 24 months, there was no difference in BPAR (22.7% EVR vs. 19.1% CNI, <i>p</i> = 0.63). Median eGFR at 24 months posttransplant was not significantly different (68.6 [24.8 to 112.4] mL/min EVR vs. 75.9 [35.6–116.2] mL/min CNI, <i>p</i> = 0.103). Change in eGFR from baseline was worse in the EVR group (−13.0 [−39.9 to 13.9] mL/min EVR vs. −5.0 [−31.2 to 21.2] mL/min CNI, <i>p</i> = 0.047). Median change from conversion to 24 months posttransplant (EVR group only) was −3.43 mL/min/1.73 m<sup>2</sup> (−21.0 to 9.6).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Early EVR conversion was not associated with increased risk of rejection among LDLT recipients. Renal function was not impacted. EVR may be considered as an alternative after LDLT in patients intolerant of CNIs.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"38 7","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2024-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15402","citationCount":"0","resultStr":"{\"title\":\"Early Conversion to Everolimus Within 180 Days of Living Donor Liver Transplantation\",\"authors\":\"Katelyn N. Rudzik, Kristine S. Schonder, Abhinav Humar, Heather J. Johnson\",\"doi\":\"10.1111/ctr.15402\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Early conversion to Everolimus (EVR) post deceased donor liver transplant has been associated with improved renal function but increased rejection. Early EVR conversion has not been evaluated after living donor liver transplant (LDLT). A retrospective cohort study was conducted to compare the rate of rejection and renal function in patients converted to EVR early post-LDLT to patients on calcineurin inhibitors (CNIs).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a single center retrospective cohort study of adult LDLT recipients between January 2012 and July 2019. Patients converted to EVR within 180 days of transplant were compared to patients on CNIs. The primary endpoint was biopsy proven acute rejection (BPAR) at 24 months posttransplant. Key secondary endpoints included eGFR at 24 months, change in eGFR, adverse events, and all-cause mortality.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>From a total of 173 patients involved in the study: 58 were included in the EVR group and 115 in the CNI group. Median conversion to EVR was 26 days post-LDLT. At 24 months, there was no difference in BPAR (22.7% EVR vs. 19.1% CNI, <i>p</i> = 0.63). Median eGFR at 24 months posttransplant was not significantly different (68.6 [24.8 to 112.4] mL/min EVR vs. 75.9 [35.6–116.2] mL/min CNI, <i>p</i> = 0.103). Change in eGFR from baseline was worse in the EVR group (−13.0 [−39.9 to 13.9] mL/min EVR vs. −5.0 [−31.2 to 21.2] mL/min CNI, <i>p</i> = 0.047). Median change from conversion to 24 months posttransplant (EVR group only) was −3.43 mL/min/1.73 m<sup>2</sup> (−21.0 to 9.6).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Early EVR conversion was not associated with increased risk of rejection among LDLT recipients. Renal function was not impacted. EVR may be considered as an alternative after LDLT in patients intolerant of CNIs.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10467,\"journal\":{\"name\":\"Clinical Transplantation\",\"volume\":\"38 7\",\"pages\":\"\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.15402\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15402\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.15402","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Early Conversion to Everolimus Within 180 Days of Living Donor Liver Transplantation
Background
Early conversion to Everolimus (EVR) post deceased donor liver transplant has been associated with improved renal function but increased rejection. Early EVR conversion has not been evaluated after living donor liver transplant (LDLT). A retrospective cohort study was conducted to compare the rate of rejection and renal function in patients converted to EVR early post-LDLT to patients on calcineurin inhibitors (CNIs).
Methods
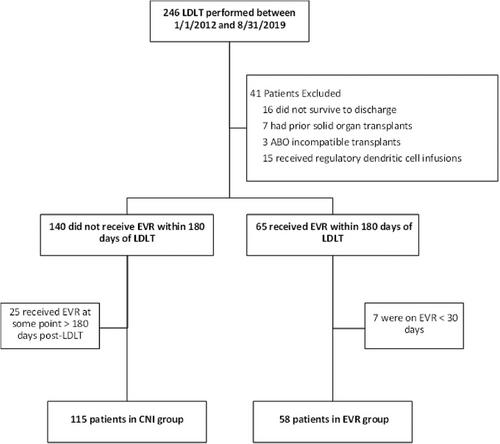
This was a single center retrospective cohort study of adult LDLT recipients between January 2012 and July 2019. Patients converted to EVR within 180 days of transplant were compared to patients on CNIs. The primary endpoint was biopsy proven acute rejection (BPAR) at 24 months posttransplant. Key secondary endpoints included eGFR at 24 months, change in eGFR, adverse events, and all-cause mortality.
Results
From a total of 173 patients involved in the study: 58 were included in the EVR group and 115 in the CNI group. Median conversion to EVR was 26 days post-LDLT. At 24 months, there was no difference in BPAR (22.7% EVR vs. 19.1% CNI, p = 0.63). Median eGFR at 24 months posttransplant was not significantly different (68.6 [24.8 to 112.4] mL/min EVR vs. 75.9 [35.6–116.2] mL/min CNI, p = 0.103). Change in eGFR from baseline was worse in the EVR group (−13.0 [−39.9 to 13.9] mL/min EVR vs. −5.0 [−31.2 to 21.2] mL/min CNI, p = 0.047). Median change from conversion to 24 months posttransplant (EVR group only) was −3.43 mL/min/1.73 m2 (−21.0 to 9.6).
Conclusions
Early EVR conversion was not associated with increased risk of rejection among LDLT recipients. Renal function was not impacted. EVR may be considered as an alternative after LDLT in patients intolerant of CNIs.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
