{"title":"在良性胰管狭窄中移除嵌入式全覆盖自膨胀金属支架的 \"SEMS-in-SEMS \"技术。","authors":"Il Sang Shin, Jong Ho Moon, Yun Nah Lee","doi":"10.1111/den.14887","DOIUrl":null,"url":null,"abstract":"<p>Fully covered self-expandable metal stents (SEMS) are an alternative treatment option for persistent benign main pancreatic duct stricture (BPS), but their removal can be hampered by fibrosis formation and tissue overgrowth if the indwelling duration exceeds 3 months.<span><sup>1</sup></span> We present a case in which a fully covered SEMS, which initially could not be removed from the pancreatic duct, was retrieved using a “SEMS-in-SEMS” technique.</p><p>A 69-year-old male patient with a history of symptomatic chronic pancreatitis treated by multiple exchanges of plastic stents presented with abdominal pain. Computed tomography identified refractory BPS at the pancreatic head, and a fully covered SEMS (Bonastent M-intraductal; Standard Sci Tech, Seoul, South Korea) with a diameter of 8 mm and a length of 5 cm was inserted across the stricture. Although stent removal and a follow-up pancreatogram were scheduled at 3 months, the patient arbitrarily delayed visiting the hospital until 7 months after SEMS insertion. During the delayed follow-up endoscopic retrograde cholangiopancreatography, the inserted SEMS could not be removed, likely because it had become embedded in the pancreatic duct wall. Subsequent pancreatogram suggested tissue hyperplasia and overgrowth into the stent. The SEMS-in-SEMS technique was performed by placing a second fully covered SEMS with a diameter of 10 mm and a length of 7 cm, extended by 1 cm at both ends, inside the existing SEMS to compress the hyperplastic tissue and induce its ischemia and necrosis (Fig. 1, Video S1). One month later, an attempt to remove both stents using a rat-tooth forceps succeeded (Fig. 2).</p><p>The placement of a SEMS inside another SEMS can induce pressure necrosis of bile duct hyperplasia, enabling subsequent removal of the embedded biliary stent.<span><sup>2-4</sup></span> The SEMS-in-SEMS technique, which was documented only in the bile duct interventions, can also be safe and effective for the extraction of embedded SEMS in patients with BPS.</p><p>Authors declare no conflict of interest for this article.</p><p>This work was partly supported by the SoonChunHyang University Research Fund.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 10","pages":"1171-1172"},"PeriodicalIF":4.7000,"publicationDate":"2024-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14887","citationCount":"0","resultStr":"{\"title\":\"“SEMS-in-SEMS” technique for the removal of embedded fully covered self-expandable metal stents in benign pancreatic duct stricture\",\"authors\":\"Il Sang Shin, Jong Ho Moon, Yun Nah Lee\",\"doi\":\"10.1111/den.14887\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Fully covered self-expandable metal stents (SEMS) are an alternative treatment option for persistent benign main pancreatic duct stricture (BPS), but their removal can be hampered by fibrosis formation and tissue overgrowth if the indwelling duration exceeds 3 months.<span><sup>1</sup></span> We present a case in which a fully covered SEMS, which initially could not be removed from the pancreatic duct, was retrieved using a “SEMS-in-SEMS” technique.</p><p>A 69-year-old male patient with a history of symptomatic chronic pancreatitis treated by multiple exchanges of plastic stents presented with abdominal pain. Computed tomography identified refractory BPS at the pancreatic head, and a fully covered SEMS (Bonastent M-intraductal; Standard Sci Tech, Seoul, South Korea) with a diameter of 8 mm and a length of 5 cm was inserted across the stricture. Although stent removal and a follow-up pancreatogram were scheduled at 3 months, the patient arbitrarily delayed visiting the hospital until 7 months after SEMS insertion. During the delayed follow-up endoscopic retrograde cholangiopancreatography, the inserted SEMS could not be removed, likely because it had become embedded in the pancreatic duct wall. Subsequent pancreatogram suggested tissue hyperplasia and overgrowth into the stent. The SEMS-in-SEMS technique was performed by placing a second fully covered SEMS with a diameter of 10 mm and a length of 7 cm, extended by 1 cm at both ends, inside the existing SEMS to compress the hyperplastic tissue and induce its ischemia and necrosis (Fig. 1, Video S1). One month later, an attempt to remove both stents using a rat-tooth forceps succeeded (Fig. 2).</p><p>The placement of a SEMS inside another SEMS can induce pressure necrosis of bile duct hyperplasia, enabling subsequent removal of the embedded biliary stent.<span><sup>2-4</sup></span> The SEMS-in-SEMS technique, which was documented only in the bile duct interventions, can also be safe and effective for the extraction of embedded SEMS in patients with BPS.</p><p>Authors declare no conflict of interest for this article.</p><p>This work was partly supported by the SoonChunHyang University Research Fund.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 10\",\"pages\":\"1171-1172\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-07-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14887\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14887\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14887","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
“SEMS-in-SEMS” technique for the removal of embedded fully covered self-expandable metal stents in benign pancreatic duct stricture
Fully covered self-expandable metal stents (SEMS) are an alternative treatment option for persistent benign main pancreatic duct stricture (BPS), but their removal can be hampered by fibrosis formation and tissue overgrowth if the indwelling duration exceeds 3 months.1 We present a case in which a fully covered SEMS, which initially could not be removed from the pancreatic duct, was retrieved using a “SEMS-in-SEMS” technique.
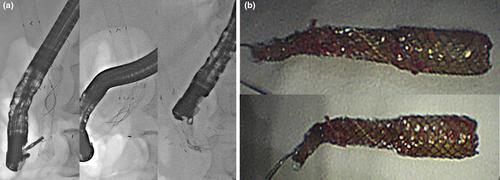
A 69-year-old male patient with a history of symptomatic chronic pancreatitis treated by multiple exchanges of plastic stents presented with abdominal pain. Computed tomography identified refractory BPS at the pancreatic head, and a fully covered SEMS (Bonastent M-intraductal; Standard Sci Tech, Seoul, South Korea) with a diameter of 8 mm and a length of 5 cm was inserted across the stricture. Although stent removal and a follow-up pancreatogram were scheduled at 3 months, the patient arbitrarily delayed visiting the hospital until 7 months after SEMS insertion. During the delayed follow-up endoscopic retrograde cholangiopancreatography, the inserted SEMS could not be removed, likely because it had become embedded in the pancreatic duct wall. Subsequent pancreatogram suggested tissue hyperplasia and overgrowth into the stent. The SEMS-in-SEMS technique was performed by placing a second fully covered SEMS with a diameter of 10 mm and a length of 7 cm, extended by 1 cm at both ends, inside the existing SEMS to compress the hyperplastic tissue and induce its ischemia and necrosis (Fig. 1, Video S1). One month later, an attempt to remove both stents using a rat-tooth forceps succeeded (Fig. 2).
The placement of a SEMS inside another SEMS can induce pressure necrosis of bile duct hyperplasia, enabling subsequent removal of the embedded biliary stent.2-4 The SEMS-in-SEMS technique, which was documented only in the bile duct interventions, can also be safe and effective for the extraction of embedded SEMS in patients with BPS.
Authors declare no conflict of interest for this article.
This work was partly supported by the SoonChunHyang University Research Fund.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
