Pierre Arnautou , Guillaume Garnier , Jean Maillot , Johanna Konopacki , Michel Brachet , Annabelle Bonnin , Jean-Christophe Amabile , Jean-Valère Malfuson
{"title":"急性辐射综合征的处理。","authors":"Pierre Arnautou , Guillaume Garnier , Jean Maillot , Johanna Konopacki , Michel Brachet , Annabelle Bonnin , Jean-Christophe Amabile , Jean-Valère Malfuson","doi":"10.1016/j.tracli.2024.07.002","DOIUrl":null,"url":null,"abstract":"<div><div>Acute radiation syndrome encompasses a spectrum of pathological manifestations resulting from exposure to high doses of ionizing radiation. This syndrome typically progresses through three stages with a prodromal phase, a latency phase and a critical phase. Each of them varies in intensity and duration depending on the absorbed dose of radiation. Predominantly affecting the bone marrow, skin, and gastrointestinal tract, its clinical implications are profound and multiorgan failure must be considered. Radiation doses below 2 Gray generally result in insignificant clinical consequences, while exposures surpassing 12 Gray exceeds current therapeutic capacities.</div><div>Survival outcomes for patients within this therapeutic range depend on their ability to withstand radiation-induced aplasia, compounded by an increased risk of bleeding and infection due to skin, gastrointestinal, and potentially combined radiation injuries.</div><div>Assessing the degree of radiation exposure plays a pivotal role in tailoring patient management strategies and is based on a combination of clinical, biological, and physical parameters. Treatment approaches primarily include intensive hematologic support to manage symptomatic manifestations and etiologic treatment is now based on the administration of growth factors.</div><div>The role of hematopoietic stem cell transplant (HSCT) will be carefully considered on an individual basis, especially for patients who do not respond following 3 weeks of cytokine therapy.</div><div>This review highlights the pathophysiological mechanisms, assessment modalities, and therapeutic interventions crucial for managing acute radiation syndrome aiming to optimize patient outcomes and guide clinical practice.</div></div>","PeriodicalId":23262,"journal":{"name":"Transfusion Clinique et Biologique","volume":"31 4","pages":"Pages 253-259"},"PeriodicalIF":1.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Management of acute radiation syndrome\",\"authors\":\"Pierre Arnautou , Guillaume Garnier , Jean Maillot , Johanna Konopacki , Michel Brachet , Annabelle Bonnin , Jean-Christophe Amabile , Jean-Valère Malfuson\",\"doi\":\"10.1016/j.tracli.2024.07.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><div>Acute radiation syndrome encompasses a spectrum of pathological manifestations resulting from exposure to high doses of ionizing radiation. This syndrome typically progresses through three stages with a prodromal phase, a latency phase and a critical phase. Each of them varies in intensity and duration depending on the absorbed dose of radiation. Predominantly affecting the bone marrow, skin, and gastrointestinal tract, its clinical implications are profound and multiorgan failure must be considered. Radiation doses below 2 Gray generally result in insignificant clinical consequences, while exposures surpassing 12 Gray exceeds current therapeutic capacities.</div><div>Survival outcomes for patients within this therapeutic range depend on their ability to withstand radiation-induced aplasia, compounded by an increased risk of bleeding and infection due to skin, gastrointestinal, and potentially combined radiation injuries.</div><div>Assessing the degree of radiation exposure plays a pivotal role in tailoring patient management strategies and is based on a combination of clinical, biological, and physical parameters. Treatment approaches primarily include intensive hematologic support to manage symptomatic manifestations and etiologic treatment is now based on the administration of growth factors.</div><div>The role of hematopoietic stem cell transplant (HSCT) will be carefully considered on an individual basis, especially for patients who do not respond following 3 weeks of cytokine therapy.</div><div>This review highlights the pathophysiological mechanisms, assessment modalities, and therapeutic interventions crucial for managing acute radiation syndrome aiming to optimize patient outcomes and guide clinical practice.</div></div>\",\"PeriodicalId\":23262,\"journal\":{\"name\":\"Transfusion Clinique et Biologique\",\"volume\":\"31 4\",\"pages\":\"Pages 253-259\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transfusion Clinique et Biologique\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1246782024000922\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transfusion Clinique et Biologique","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1246782024000922","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/16 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
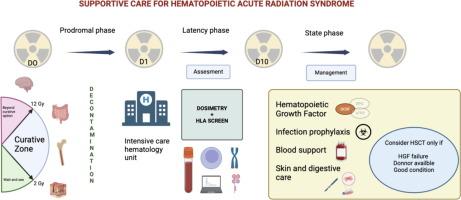
Acute radiation syndrome encompasses a spectrum of pathological manifestations resulting from exposure to high doses of ionizing radiation. This syndrome typically progresses through three stages with a prodromal phase, a latency phase and a critical phase. Each of them varies in intensity and duration depending on the absorbed dose of radiation. Predominantly affecting the bone marrow, skin, and gastrointestinal tract, its clinical implications are profound and multiorgan failure must be considered. Radiation doses below 2 Gray generally result in insignificant clinical consequences, while exposures surpassing 12 Gray exceeds current therapeutic capacities.
Survival outcomes for patients within this therapeutic range depend on their ability to withstand radiation-induced aplasia, compounded by an increased risk of bleeding and infection due to skin, gastrointestinal, and potentially combined radiation injuries.
Assessing the degree of radiation exposure plays a pivotal role in tailoring patient management strategies and is based on a combination of clinical, biological, and physical parameters. Treatment approaches primarily include intensive hematologic support to manage symptomatic manifestations and etiologic treatment is now based on the administration of growth factors.
The role of hematopoietic stem cell transplant (HSCT) will be carefully considered on an individual basis, especially for patients who do not respond following 3 weeks of cytokine therapy.
This review highlights the pathophysiological mechanisms, assessment modalities, and therapeutic interventions crucial for managing acute radiation syndrome aiming to optimize patient outcomes and guide clinical practice.
期刊介绍:
Transfusion Clinique et Biologique, the official journal of the French Society of Blood Transfusion (SFTS):
- an aid to training, at a European level
- the only French journal indexed in the hematology and immunology sections of Current Contents
Transfusion Clinique et Biologique spans fundamental research and everyday practice, with articles coming from both sides. Articles, reviews, case reports, letters to the editor and editorials are published in 4 editions a year, in French or in English, covering all scientific and medical aspects of transfusion: immunology, hematology, infectious diseases, genetics, molecular biology, etc. And finally, a convivial cross-disciplinary section on training and information offers practical updates.
Readership:
"Transfusers" are many and various: anesthetists, biologists, hematologists, and blood-bank, ICU and mobile emergency specialists...



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
