{"title":"印度心血管质量改进战略随机对照试验的原理、设计和基线特征:C-QIP 试验。","authors":"Kavita Singh PhD , Kalyani Nikhare BDS, MPH , Mareesha Gandral BDS, MPH , Kiran Aithal MD , Satish G. Patil PhD , Girish MP MD, DM , Mohit Gupta MD, DM , Kushal Madan PhD , J.P.S. Sawhney DM , Kamar Ali BTech , Dimple Kondal PhD , Devraj Jindal BDS, MPH , Emily Mendenhall PhD , Shivani A. Patel PhD , K.M. Venkat Narayan MD, MSC, MBA , Nikhil Tandon MD, PhD , Ambuj Roy MD, DM , Mark D. Huffman MD, MPH , Dorairaj Prabhakaran MD, DM","doi":"10.1016/j.ahj.2024.07.008","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Quality of chronic care for cardiovascular disease (CVD) remains suboptimal worldwide. The Collaborative Quality ImProvement (C-QIP) trial aims to develop and test the feasibility and clinical effect of a multicomponent strategy among patients with prevalent CVD in India.</p></div><div><h3>Methods</h3><p>The C-QIP is a clinic-based, open randomized trial of a multicomponent intervention vs usual care that was locally developed and adapted for use in Indian settings through rigorous formative research guided by Consolidated Framework for Implementation Research (CFIR). The C-QIP intervention consisted of 5 components: 1) electronic health records and decision support system for clinicians, 2) trained nonphysician health workers (NPHW), 3) text-message based lifestyle reminders, 4) patient education materials, 5) quarterly audit and feedback reports. Patients with CVD (ischemic heart disease, ischemic stroke, or heart failure) attending outpatient CVD clinics were recruited from September 2022 to September 2023 and were randomized to the intervention or usual care arm for at least 12 months follow-up. The co-primary outcomes are implementation feasibility, fidelity (ie, dose delivered and dose received), acceptability, adoption and appropriateness, measured at multiple levels: patient, provider and clinic site-level, The secondary outcomes include prescription of guideline directed medical therapy (GDMT) (provider-level), and adherence to prescribed therapy, change in mean blood pressure (BP) and LDL-cholesterol between the intervention and control groups (patient-level). In addition, a trial-based process and economic evaluations will be performed using standard guidelines.</p></div><div><h3>Results</h3><p>We recruited 410 socio-demographically diverse patients with CVD from 4 hospitals in India. Mean (SD) age was 57.5 (11.7) years, and 73.0% were males. Self-reported history of hypertension (48.5%) and diabetes (41.5%) was common. At baseline, mean (SD) BP was 127.9 (18.2) /76.2 (11.6) mm Hg, mean (SD) LDLc: 80.3 (37.3) mg/dl and mean (SD) HbA1c: 6.8% (1.6%). At baseline, the GDMT varied from 62.4% for patients with ischemic heart disease, 48.6% for ischemic stroke and 36.1% for heart failure.</p></div><div><h3>Conclusion</h3><p>This study will establish the feasibility of delivering contextually relevant, and evidence-based C-QIP strategy and assess whether it is acceptable to the target populations. The study results will inform a larger scale confirmatory trial of a comprehensive CVD care model in low-resource settings.</p></div><div><h3>Trial registration</h3><p>Clinical Trials Registry India: CTRI/2022/04/041847; Clinicaltrials.gov number: NCT05196659.</p></div>","PeriodicalId":7868,"journal":{"name":"American heart journal","volume":"276 ","pages":"Pages 83-98"},"PeriodicalIF":3.5000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Rationale, Design and Baseline Characteristics of a Randomized Controlled Trial of a Cardiovascular Quality Improvement Strategy in India: The C-QIP Trial\",\"authors\":\"Kavita Singh PhD , Kalyani Nikhare BDS, MPH , Mareesha Gandral BDS, MPH , Kiran Aithal MD , Satish G. Patil PhD , Girish MP MD, DM , Mohit Gupta MD, DM , Kushal Madan PhD , J.P.S. Sawhney DM , Kamar Ali BTech , Dimple Kondal PhD , Devraj Jindal BDS, MPH , Emily Mendenhall PhD , Shivani A. Patel PhD , K.M. Venkat Narayan MD, MSC, MBA , Nikhil Tandon MD, PhD , Ambuj Roy MD, DM , Mark D. Huffman MD, MPH , Dorairaj Prabhakaran MD, DM\",\"doi\":\"10.1016/j.ahj.2024.07.008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Quality of chronic care for cardiovascular disease (CVD) remains suboptimal worldwide. The Collaborative Quality ImProvement (C-QIP) trial aims to develop and test the feasibility and clinical effect of a multicomponent strategy among patients with prevalent CVD in India.</p></div><div><h3>Methods</h3><p>The C-QIP is a clinic-based, open randomized trial of a multicomponent intervention vs usual care that was locally developed and adapted for use in Indian settings through rigorous formative research guided by Consolidated Framework for Implementation Research (CFIR). The C-QIP intervention consisted of 5 components: 1) electronic health records and decision support system for clinicians, 2) trained nonphysician health workers (NPHW), 3) text-message based lifestyle reminders, 4) patient education materials, 5) quarterly audit and feedback reports. Patients with CVD (ischemic heart disease, ischemic stroke, or heart failure) attending outpatient CVD clinics were recruited from September 2022 to September 2023 and were randomized to the intervention or usual care arm for at least 12 months follow-up. The co-primary outcomes are implementation feasibility, fidelity (ie, dose delivered and dose received), acceptability, adoption and appropriateness, measured at multiple levels: patient, provider and clinic site-level, The secondary outcomes include prescription of guideline directed medical therapy (GDMT) (provider-level), and adherence to prescribed therapy, change in mean blood pressure (BP) and LDL-cholesterol between the intervention and control groups (patient-level). In addition, a trial-based process and economic evaluations will be performed using standard guidelines.</p></div><div><h3>Results</h3><p>We recruited 410 socio-demographically diverse patients with CVD from 4 hospitals in India. Mean (SD) age was 57.5 (11.7) years, and 73.0% were males. Self-reported history of hypertension (48.5%) and diabetes (41.5%) was common. At baseline, mean (SD) BP was 127.9 (18.2) /76.2 (11.6) mm Hg, mean (SD) LDLc: 80.3 (37.3) mg/dl and mean (SD) HbA1c: 6.8% (1.6%). At baseline, the GDMT varied from 62.4% for patients with ischemic heart disease, 48.6% for ischemic stroke and 36.1% for heart failure.</p></div><div><h3>Conclusion</h3><p>This study will establish the feasibility of delivering contextually relevant, and evidence-based C-QIP strategy and assess whether it is acceptable to the target populations. The study results will inform a larger scale confirmatory trial of a comprehensive CVD care model in low-resource settings.</p></div><div><h3>Trial registration</h3><p>Clinical Trials Registry India: CTRI/2022/04/041847; Clinicaltrials.gov number: NCT05196659.</p></div>\",\"PeriodicalId\":7868,\"journal\":{\"name\":\"American heart journal\",\"volume\":\"276 \",\"pages\":\"Pages 83-98\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American heart journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0002870324001741\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American heart journal","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0002870324001741","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Rationale, Design and Baseline Characteristics of a Randomized Controlled Trial of a Cardiovascular Quality Improvement Strategy in India: The C-QIP Trial
Background
Quality of chronic care for cardiovascular disease (CVD) remains suboptimal worldwide. The Collaborative Quality ImProvement (C-QIP) trial aims to develop and test the feasibility and clinical effect of a multicomponent strategy among patients with prevalent CVD in India.
Methods
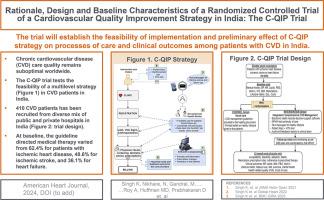
The C-QIP is a clinic-based, open randomized trial of a multicomponent intervention vs usual care that was locally developed and adapted for use in Indian settings through rigorous formative research guided by Consolidated Framework for Implementation Research (CFIR). The C-QIP intervention consisted of 5 components: 1) electronic health records and decision support system for clinicians, 2) trained nonphysician health workers (NPHW), 3) text-message based lifestyle reminders, 4) patient education materials, 5) quarterly audit and feedback reports. Patients with CVD (ischemic heart disease, ischemic stroke, or heart failure) attending outpatient CVD clinics were recruited from September 2022 to September 2023 and were randomized to the intervention or usual care arm for at least 12 months follow-up. The co-primary outcomes are implementation feasibility, fidelity (ie, dose delivered and dose received), acceptability, adoption and appropriateness, measured at multiple levels: patient, provider and clinic site-level, The secondary outcomes include prescription of guideline directed medical therapy (GDMT) (provider-level), and adherence to prescribed therapy, change in mean blood pressure (BP) and LDL-cholesterol between the intervention and control groups (patient-level). In addition, a trial-based process and economic evaluations will be performed using standard guidelines.
Results
We recruited 410 socio-demographically diverse patients with CVD from 4 hospitals in India. Mean (SD) age was 57.5 (11.7) years, and 73.0% were males. Self-reported history of hypertension (48.5%) and diabetes (41.5%) was common. At baseline, mean (SD) BP was 127.9 (18.2) /76.2 (11.6) mm Hg, mean (SD) LDLc: 80.3 (37.3) mg/dl and mean (SD) HbA1c: 6.8% (1.6%). At baseline, the GDMT varied from 62.4% for patients with ischemic heart disease, 48.6% for ischemic stroke and 36.1% for heart failure.
Conclusion
This study will establish the feasibility of delivering contextually relevant, and evidence-based C-QIP strategy and assess whether it is acceptable to the target populations. The study results will inform a larger scale confirmatory trial of a comprehensive CVD care model in low-resource settings.
期刊介绍:
The American Heart Journal will consider for publication suitable articles on topics pertaining to the broad discipline of cardiovascular disease. Our goal is to provide the reader primary investigation, scholarly review, and opinion concerning the practice of cardiovascular medicine. We especially encourage submission of 3 types of reports that are not frequently seen in cardiovascular journals: negative clinical studies, reports on study designs, and studies involving the organization of medical care. The Journal does not accept individual case reports or original articles involving bench laboratory or animal research.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
