{"title":"慢性淋巴细胞白血病前期固定疗程疗法的网络荟萃分析。","authors":"Stefano Molica, David Allsup, Diana Giannarelli","doi":"10.1002/ajh.27437","DOIUrl":null,"url":null,"abstract":"<p>The emergence of Bruton's tyrosine kinase (BTK) inhibitors marked a significant advancement in chronic lymphocytic leukemia (CLL) management, especially for high-risk patients.<span><sup>1</sup></span> Ibrutinib, the pioneering BTK inhibitor, has undergone extensive study. The final analysis of the RESONATE-2 study confirms its sustained survival benefit for first-line CLL treatment with up to 10 years of follow-up.<span><sup>2</sup></span> Despite its efficacy, prolonged administration of BTK inhibitors can lead to cardiovascular toxicities and emergence of therapy resistance mutations.<span><sup>3, 4</sup></span></p><p>Time-limited CLL-directed therapies, inspired by venetoclax's unique attributes in inducing deep therapeutic responses, aim to address continuous therapy limitations.<span><sup>5</sup></span> Venetoclax combined with anti-CD20 monoclonal antibodies in fixed-duration (FD) regimens, showcased in relapsed/refractory CLL with MURANO and in frontline with CLL14 and CLL13 trials, sustain responses with manageable toxicity across CLL patient profiles.<span><sup>6-9</sup></span></p><p>By harnessing the synergistic potential of venetoclax and ibrutinib (VI), which combines agents with distinct mechanisms of action and non-overlapping toxicities, researchers aim to attain deeper and persistent treatment responses without associated therapy resistance.<span><sup>10-14</sup></span> This combination has recently received approval from the European Medicines Agency (EMA) for frontline treatment of CLL.<span><sup>15</sup></span> This approval is based on pivotal findings from the Phase 3 GLOW study, which demonstrated superior PFS in patients treated with VI compared with those treated with chlorambucil-obinutuzumab, and from the FD cohort of the Phase 2 CAPTIVATE study.<span><sup>10, 11</sup></span> However, the choice between FD therapies remains challenging due to the lack of head-to-head comparative data. Results from the ongoing CLL17 trial (NCT04608318), which is comparing continuous BTK inhibitor therapy with FD regimens, including VI and venetoclax-obinutuzumab (VO), are eagerly anticipated.</p><p>To provisionally support evidence-based decision-making, we performed a network meta-analysis (NMA) comparing all approved FD therapies in the setting of treatment-naïve (TN) CLL patients.</p><p>Relevant randomized clinical trials were identified through a systematic review of the literature in MEDLINE. To be included, studies had to meet the following criteria: (1) to be randomized controlled trials (RCTs) focusing on FD therapy in TN CLL patients; (2) to investigate the effectiveness of FD therapy with venetoclax as its core component; and (3) to provide data on both progression-free survival (PFS) and overall survival (OS). Reporting of the systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.<span><sup>16</sup></span> Two reviewers (S.M. and D.G.) independently assessed the eligibility of all identified citations and extracted data from original trial reports. Consistent efficacy endpoints, such as PFS and OS, were extracted and synthesized in the random effects NMA. The quality and certainty of the evidence for all outcomes with sufficient data were assessed using the recommended strategies developed by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) working group<span><sup>17</sup></span> (Supplementary Materials). A graphical method was employed to visually synthesize the experimental evidence by presenting the hazard ratio (HR) values of direct and indirect comparisons. A treatment was considered more effective than another if the 95% confidence interval (CI) for HR did not encompass the value 1.0 (which corresponds to a Bayesian probability of <i>p</i> <span></span><math>\n <mrow>\n <mo>≥</mo>\n </mrow></math> 97.5% for this pairwise comparison).</p><p>Four RCTs were identified as suitable for inclusion in the base-case network analysis (Supplementary Figure 1).<span><sup>7, 11, 12, 18</sup></span> Data with the longest available median follow-up were utilized: CLL14, 76.4 months; GLOW, 57 months; FLAIR, 43.7 months; CLL13, 50.7 months.<span><sup>9, 12, 19, 20</sup></span></p><p>Supplementary Table 1 provides the main clinical and biological characteristics of patients enrolled in these trials. CLL13 and FLAIR recruited younger and fitter patients, whereas CLL14 and GLOW enrolled elderly and less fit individuals.<span><sup>7, 11, 12, 18</sup></span> However, upon stratification of the data by patient age and fitness, some heterogeneity across the trials was observed. This heterogeneity was primarily attributable to a higher proportion of patients with a Cumulative Illness Rating Scale (CIRS) score greater than 6 in the CLL14 trial compared with the GLOW trial (<i>p</i> = .0004). Additionally, there was a higher prevalence of patients with unmutated immunoglobulin heavy-chain variable region (<i>IGHV</i>) gene in the CLL13 trial compared with the FLAIR trial (<i>p</i> = .03) (Supplementary Table 1).</p><p>The trial analysis group consisted of 1.632 patients, with 819 (50.1%) receiving FD treatment with targeted agents and 813 (49.8%) receiving chemoimmunotherapy (CIT). Targeted agent arms evaluated VI combination in 366 (44.6%) cases (from the GLOW and FLAIR trials), and VO combination in 453 (55.3%) cases (from the CLL14 and CLL13 trials). The control arms of the RCTs employed CIT with varying intensities, reflecting differences in patient age and fitness status. Specifically, the control arms for the CLL14 and GLOW trials consisted of chlorambucil and obinutuzumab in 321 (39.4%) cases. Meanwhile, 492 (60.5%) younger and fit patients received fludarabine, cyclophosphamide, and rituximab (FCR) in the control arms of the CLL13 and FLAIR trials. Notably, of 229 patients in the CIT control arm of the CLL13 trial, 79 (34.5%) received bendamustine and rituximab (BR). However, the results of the CLL13 trial were presented in aggregate form, thereby precluding separate analysis of patients treated with BR.<span><sup>18</sup></span></p><p>We initially analyzed the survival outcomes of patients pooled into two therapeutic groups irrespective of age and fitness status: VI (including GLOW and FLAIR studies) and VO (encompassing CLL13 and CLL14 studies). The HR values (HR 2.07; 95% CI, 1.35–2.16) suggest a twofold shorter PFS among patients treated with VO compared with those treated with VI (Figure 1A). In contrast, OS analysis did not reveal any statistically significant difference between the two venetoclax-based FD therapy groups (HR 1.69; 95% CI, 0.93–3.00) (Figure 1A).</p><p>To account for variability in the inclusion criteria across trials, particularly regarding age and comorbidities, the NMA was repeated with a focus upon trials that either recruited elderly or younger patients with CLL. Among younger, fitter patients enrolled in CLL13 and FLAIR trials, there was a significant worsening in PFS with the VO combination compared with VI (HR = 3.23, 95% CI: 1.54–6.78) (Figure 1B). However, in trials predominantly involving elderly or unfit patients (CLL14 and GLOW), PFS analysis failed to demonstrated statistical significance (HR = 1.67; 95% CI: 1.00–2.79) between VI and VO regimens (Figure 1B). Nonetheless, a favorable trend towards VI was apparent as the 95% CI for the HR approached but did not cross 1.00. Finally, in the OS analysis, both VI and VO equally impacted OS in younger/fit (HR = 1.87; 95% CI, 0.64–5.46) and elderly/unfit (HR = 1.47; 95% CI, 0.70–3.11) patients with CLL (Figure 1C).</p><p>Next, we investigated whether VI could exert a differential impact on PFS among unmutated <i>IGHV</i> CLL patients. Pooling together younger and elderly CLL patients, our analysis did not reveal any PFS advantage associated with the VI combination compared with VO (HR = 1.69; 95% CI, 0.94–3.03) (Figure 1A). Subsequently, in an age- and fitness-controlled analysis, younger patients (from the FLAIR and CLL13 trials) demonstrated a substantial PFS benefit with VI (HR = 6.46; 95% CI: 1.96–21.08), whereas elderly patients (from the GLOW and CLL14 trials) did not sustain this benefit (HR = 1.00; 95% CI: 0.50–1.99) (Figure 1D).</p><p>The results of this NMA definitely demonstrate improved PFS with VI compared to VO in all CLL patients, regardless of age and fitness status. This improvement is notably more pronounced among younger and fitter patients. The unique design of the FLAIR trial, involving younger/fit patients, may have influenced these findings. In this trial the duration of VI therapy depended on measurable residual disease (MRD) assessment in peripheral blood and bone marrow, potentially resulting in prolonged treatment exposure. Consequently, a significant proportion of patients discontinued VI therapy by 2 years (28.9%) and 3 years (58.0%) in the FLAIR trial,<span><sup>12</sup></span> contrasting with the fixed 12-month duration of VO combination therapy in patients enrolled in the CLL13 trial.<span><sup>18</sup></span></p><p>An anchored matching-adjusted indirect comparison (MAIC), presented at the 2024 European Hematological Association (EHA) meeting, evaluated the comparative efficacy of VI versus VO in elderly, medically unfit patients, from the GLOW and CLL14 trials.<span><sup>21</sup></span> This analysis revealed that VI consistently improved all relative treatment effects, including PFS, OS, and time to next treatment (TTNT), compared with VO. Although such an analysis confirms the PFS improvement we have observed with VI in elderly and unfit CLL patients, discrepancies in methodologies used (MAIC vs. NMA) may partly account for the superior OS benefits seen with VI exclusively in the study by López-Jiménez et al.<span><sup>21</sup></span> Nevertheless, despite the efficacy indications furnished by these indirect comparative analyses, the decision-making process for selecting the type of FD regimens in elderly, medically unfit, CLL patients must encompass factors such as renal or cardiovascular comorbidities, the perceived risk of tumor lysis syndrome (TLS), potential drug interactions, logistical considerations pertaining to the administration of parenteral therapies, and notably, patient preferences.<span><sup>22</sup></span></p><p>We acknowledge several limitations in our data, including the limited number of studies available and the heterogeneity among patients enrolled in the RCTs used for the NMA. These factors, coupled with the absence of direct comparison data, contribute to the “moderate” level of evidence assigned by GRADE to our NMA.<span><sup>17</sup></span> However, as we await the results of CLL17, which will address the question of FD regimen selection within an RCT, our analyses, though provisional, may offer valuable insights for clinical practice. Furthermore, ongoing Phase 3 studies such as MAJIC (NCT05057494) and CLL18 (anticipated to commence by the end of 2024), comparing VO with alternative venetoclax-based combinations involving second-generation covalent BTK inhibitors (e.g., acalabrutinib) or non-covalent BTK inhibitors (e.g., pirtobrutinib), will contribute to identifying the most effective FD regimen in CLL.</p><p>Stefano Molica designed the study, selected and evaluated studies, performed data extraction, evaluated and interpreted results, and wrote the manuscript. David Allsup interpreted results, supported with his advice the preparation of the manuscript, and wrote the paper. Diana Giannarelli selected and evaluated studies, performed data extraction, performed statistical analyses, and evaluated the results. All authors reviewed and approved the manuscript.</p><p>SM received honoraria from Janssen, Abbvie, and AstraZeneca. DA and DG declare no competing financial interests.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"99 10","pages":"2041-2044"},"PeriodicalIF":9.9000,"publicationDate":"2024-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27437","citationCount":"0","resultStr":"{\"title\":\"Network meta-analysis of upfront fixed-duration therapies in chronic lymphocytic leukemia\",\"authors\":\"Stefano Molica, David Allsup, Diana Giannarelli\",\"doi\":\"10.1002/ajh.27437\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The emergence of Bruton's tyrosine kinase (BTK) inhibitors marked a significant advancement in chronic lymphocytic leukemia (CLL) management, especially for high-risk patients.<span><sup>1</sup></span> Ibrutinib, the pioneering BTK inhibitor, has undergone extensive study. The final analysis of the RESONATE-2 study confirms its sustained survival benefit for first-line CLL treatment with up to 10 years of follow-up.<span><sup>2</sup></span> Despite its efficacy, prolonged administration of BTK inhibitors can lead to cardiovascular toxicities and emergence of therapy resistance mutations.<span><sup>3, 4</sup></span></p><p>Time-limited CLL-directed therapies, inspired by venetoclax's unique attributes in inducing deep therapeutic responses, aim to address continuous therapy limitations.<span><sup>5</sup></span> Venetoclax combined with anti-CD20 monoclonal antibodies in fixed-duration (FD) regimens, showcased in relapsed/refractory CLL with MURANO and in frontline with CLL14 and CLL13 trials, sustain responses with manageable toxicity across CLL patient profiles.<span><sup>6-9</sup></span></p><p>By harnessing the synergistic potential of venetoclax and ibrutinib (VI), which combines agents with distinct mechanisms of action and non-overlapping toxicities, researchers aim to attain deeper and persistent treatment responses without associated therapy resistance.<span><sup>10-14</sup></span> This combination has recently received approval from the European Medicines Agency (EMA) for frontline treatment of CLL.<span><sup>15</sup></span> This approval is based on pivotal findings from the Phase 3 GLOW study, which demonstrated superior PFS in patients treated with VI compared with those treated with chlorambucil-obinutuzumab, and from the FD cohort of the Phase 2 CAPTIVATE study.<span><sup>10, 11</sup></span> However, the choice between FD therapies remains challenging due to the lack of head-to-head comparative data. Results from the ongoing CLL17 trial (NCT04608318), which is comparing continuous BTK inhibitor therapy with FD regimens, including VI and venetoclax-obinutuzumab (VO), are eagerly anticipated.</p><p>To provisionally support evidence-based decision-making, we performed a network meta-analysis (NMA) comparing all approved FD therapies in the setting of treatment-naïve (TN) CLL patients.</p><p>Relevant randomized clinical trials were identified through a systematic review of the literature in MEDLINE. To be included, studies had to meet the following criteria: (1) to be randomized controlled trials (RCTs) focusing on FD therapy in TN CLL patients; (2) to investigate the effectiveness of FD therapy with venetoclax as its core component; and (3) to provide data on both progression-free survival (PFS) and overall survival (OS). Reporting of the systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.<span><sup>16</sup></span> Two reviewers (S.M. and D.G.) independently assessed the eligibility of all identified citations and extracted data from original trial reports. Consistent efficacy endpoints, such as PFS and OS, were extracted and synthesized in the random effects NMA. The quality and certainty of the evidence for all outcomes with sufficient data were assessed using the recommended strategies developed by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) working group<span><sup>17</sup></span> (Supplementary Materials). A graphical method was employed to visually synthesize the experimental evidence by presenting the hazard ratio (HR) values of direct and indirect comparisons. A treatment was considered more effective than another if the 95% confidence interval (CI) for HR did not encompass the value 1.0 (which corresponds to a Bayesian probability of <i>p</i> <span></span><math>\\n <mrow>\\n <mo>≥</mo>\\n </mrow></math> 97.5% for this pairwise comparison).</p><p>Four RCTs were identified as suitable for inclusion in the base-case network analysis (Supplementary Figure 1).<span><sup>7, 11, 12, 18</sup></span> Data with the longest available median follow-up were utilized: CLL14, 76.4 months; GLOW, 57 months; FLAIR, 43.7 months; CLL13, 50.7 months.<span><sup>9, 12, 19, 20</sup></span></p><p>Supplementary Table 1 provides the main clinical and biological characteristics of patients enrolled in these trials. CLL13 and FLAIR recruited younger and fitter patients, whereas CLL14 and GLOW enrolled elderly and less fit individuals.<span><sup>7, 11, 12, 18</sup></span> However, upon stratification of the data by patient age and fitness, some heterogeneity across the trials was observed. This heterogeneity was primarily attributable to a higher proportion of patients with a Cumulative Illness Rating Scale (CIRS) score greater than 6 in the CLL14 trial compared with the GLOW trial (<i>p</i> = .0004). Additionally, there was a higher prevalence of patients with unmutated immunoglobulin heavy-chain variable region (<i>IGHV</i>) gene in the CLL13 trial compared with the FLAIR trial (<i>p</i> = .03) (Supplementary Table 1).</p><p>The trial analysis group consisted of 1.632 patients, with 819 (50.1%) receiving FD treatment with targeted agents and 813 (49.8%) receiving chemoimmunotherapy (CIT). Targeted agent arms evaluated VI combination in 366 (44.6%) cases (from the GLOW and FLAIR trials), and VO combination in 453 (55.3%) cases (from the CLL14 and CLL13 trials). The control arms of the RCTs employed CIT with varying intensities, reflecting differences in patient age and fitness status. Specifically, the control arms for the CLL14 and GLOW trials consisted of chlorambucil and obinutuzumab in 321 (39.4%) cases. Meanwhile, 492 (60.5%) younger and fit patients received fludarabine, cyclophosphamide, and rituximab (FCR) in the control arms of the CLL13 and FLAIR trials. Notably, of 229 patients in the CIT control arm of the CLL13 trial, 79 (34.5%) received bendamustine and rituximab (BR). However, the results of the CLL13 trial were presented in aggregate form, thereby precluding separate analysis of patients treated with BR.<span><sup>18</sup></span></p><p>We initially analyzed the survival outcomes of patients pooled into two therapeutic groups irrespective of age and fitness status: VI (including GLOW and FLAIR studies) and VO (encompassing CLL13 and CLL14 studies). The HR values (HR 2.07; 95% CI, 1.35–2.16) suggest a twofold shorter PFS among patients treated with VO compared with those treated with VI (Figure 1A). In contrast, OS analysis did not reveal any statistically significant difference between the two venetoclax-based FD therapy groups (HR 1.69; 95% CI, 0.93–3.00) (Figure 1A).</p><p>To account for variability in the inclusion criteria across trials, particularly regarding age and comorbidities, the NMA was repeated with a focus upon trials that either recruited elderly or younger patients with CLL. Among younger, fitter patients enrolled in CLL13 and FLAIR trials, there was a significant worsening in PFS with the VO combination compared with VI (HR = 3.23, 95% CI: 1.54–6.78) (Figure 1B). However, in trials predominantly involving elderly or unfit patients (CLL14 and GLOW), PFS analysis failed to demonstrated statistical significance (HR = 1.67; 95% CI: 1.00–2.79) between VI and VO regimens (Figure 1B). Nonetheless, a favorable trend towards VI was apparent as the 95% CI for the HR approached but did not cross 1.00. Finally, in the OS analysis, both VI and VO equally impacted OS in younger/fit (HR = 1.87; 95% CI, 0.64–5.46) and elderly/unfit (HR = 1.47; 95% CI, 0.70–3.11) patients with CLL (Figure 1C).</p><p>Next, we investigated whether VI could exert a differential impact on PFS among unmutated <i>IGHV</i> CLL patients. Pooling together younger and elderly CLL patients, our analysis did not reveal any PFS advantage associated with the VI combination compared with VO (HR = 1.69; 95% CI, 0.94–3.03) (Figure 1A). Subsequently, in an age- and fitness-controlled analysis, younger patients (from the FLAIR and CLL13 trials) demonstrated a substantial PFS benefit with VI (HR = 6.46; 95% CI: 1.96–21.08), whereas elderly patients (from the GLOW and CLL14 trials) did not sustain this benefit (HR = 1.00; 95% CI: 0.50–1.99) (Figure 1D).</p><p>The results of this NMA definitely demonstrate improved PFS with VI compared to VO in all CLL patients, regardless of age and fitness status. This improvement is notably more pronounced among younger and fitter patients. The unique design of the FLAIR trial, involving younger/fit patients, may have influenced these findings. In this trial the duration of VI therapy depended on measurable residual disease (MRD) assessment in peripheral blood and bone marrow, potentially resulting in prolonged treatment exposure. Consequently, a significant proportion of patients discontinued VI therapy by 2 years (28.9%) and 3 years (58.0%) in the FLAIR trial,<span><sup>12</sup></span> contrasting with the fixed 12-month duration of VO combination therapy in patients enrolled in the CLL13 trial.<span><sup>18</sup></span></p><p>An anchored matching-adjusted indirect comparison (MAIC), presented at the 2024 European Hematological Association (EHA) meeting, evaluated the comparative efficacy of VI versus VO in elderly, medically unfit patients, from the GLOW and CLL14 trials.<span><sup>21</sup></span> This analysis revealed that VI consistently improved all relative treatment effects, including PFS, OS, and time to next treatment (TTNT), compared with VO. Although such an analysis confirms the PFS improvement we have observed with VI in elderly and unfit CLL patients, discrepancies in methodologies used (MAIC vs. NMA) may partly account for the superior OS benefits seen with VI exclusively in the study by López-Jiménez et al.<span><sup>21</sup></span> Nevertheless, despite the efficacy indications furnished by these indirect comparative analyses, the decision-making process for selecting the type of FD regimens in elderly, medically unfit, CLL patients must encompass factors such as renal or cardiovascular comorbidities, the perceived risk of tumor lysis syndrome (TLS), potential drug interactions, logistical considerations pertaining to the administration of parenteral therapies, and notably, patient preferences.<span><sup>22</sup></span></p><p>We acknowledge several limitations in our data, including the limited number of studies available and the heterogeneity among patients enrolled in the RCTs used for the NMA. These factors, coupled with the absence of direct comparison data, contribute to the “moderate” level of evidence assigned by GRADE to our NMA.<span><sup>17</sup></span> However, as we await the results of CLL17, which will address the question of FD regimen selection within an RCT, our analyses, though provisional, may offer valuable insights for clinical practice. Furthermore, ongoing Phase 3 studies such as MAJIC (NCT05057494) and CLL18 (anticipated to commence by the end of 2024), comparing VO with alternative venetoclax-based combinations involving second-generation covalent BTK inhibitors (e.g., acalabrutinib) or non-covalent BTK inhibitors (e.g., pirtobrutinib), will contribute to identifying the most effective FD regimen in CLL.</p><p>Stefano Molica designed the study, selected and evaluated studies, performed data extraction, evaluated and interpreted results, and wrote the manuscript. David Allsup interpreted results, supported with his advice the preparation of the manuscript, and wrote the paper. Diana Giannarelli selected and evaluated studies, performed data extraction, performed statistical analyses, and evaluated the results. All authors reviewed and approved the manuscript.</p><p>SM received honoraria from Janssen, Abbvie, and AstraZeneca. DA and DG declare no competing financial interests.</p>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"99 10\",\"pages\":\"2041-2044\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2024-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27437\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27437\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27437","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Network meta-analysis of upfront fixed-duration therapies in chronic lymphocytic leukemia
The emergence of Bruton's tyrosine kinase (BTK) inhibitors marked a significant advancement in chronic lymphocytic leukemia (CLL) management, especially for high-risk patients.1 Ibrutinib, the pioneering BTK inhibitor, has undergone extensive study. The final analysis of the RESONATE-2 study confirms its sustained survival benefit for first-line CLL treatment with up to 10 years of follow-up.2 Despite its efficacy, prolonged administration of BTK inhibitors can lead to cardiovascular toxicities and emergence of therapy resistance mutations.3, 4
Time-limited CLL-directed therapies, inspired by venetoclax's unique attributes in inducing deep therapeutic responses, aim to address continuous therapy limitations.5 Venetoclax combined with anti-CD20 monoclonal antibodies in fixed-duration (FD) regimens, showcased in relapsed/refractory CLL with MURANO and in frontline with CLL14 and CLL13 trials, sustain responses with manageable toxicity across CLL patient profiles.6-9
By harnessing the synergistic potential of venetoclax and ibrutinib (VI), which combines agents with distinct mechanisms of action and non-overlapping toxicities, researchers aim to attain deeper and persistent treatment responses without associated therapy resistance.10-14 This combination has recently received approval from the European Medicines Agency (EMA) for frontline treatment of CLL.15 This approval is based on pivotal findings from the Phase 3 GLOW study, which demonstrated superior PFS in patients treated with VI compared with those treated with chlorambucil-obinutuzumab, and from the FD cohort of the Phase 2 CAPTIVATE study.10, 11 However, the choice between FD therapies remains challenging due to the lack of head-to-head comparative data. Results from the ongoing CLL17 trial (NCT04608318), which is comparing continuous BTK inhibitor therapy with FD regimens, including VI and venetoclax-obinutuzumab (VO), are eagerly anticipated.
To provisionally support evidence-based decision-making, we performed a network meta-analysis (NMA) comparing all approved FD therapies in the setting of treatment-naïve (TN) CLL patients.
Relevant randomized clinical trials were identified through a systematic review of the literature in MEDLINE. To be included, studies had to meet the following criteria: (1) to be randomized controlled trials (RCTs) focusing on FD therapy in TN CLL patients; (2) to investigate the effectiveness of FD therapy with venetoclax as its core component; and (3) to provide data on both progression-free survival (PFS) and overall survival (OS). Reporting of the systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.16 Two reviewers (S.M. and D.G.) independently assessed the eligibility of all identified citations and extracted data from original trial reports. Consistent efficacy endpoints, such as PFS and OS, were extracted and synthesized in the random effects NMA. The quality and certainty of the evidence for all outcomes with sufficient data were assessed using the recommended strategies developed by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) working group17 (Supplementary Materials). A graphical method was employed to visually synthesize the experimental evidence by presenting the hazard ratio (HR) values of direct and indirect comparisons. A treatment was considered more effective than another if the 95% confidence interval (CI) for HR did not encompass the value 1.0 (which corresponds to a Bayesian probability of p 97.5% for this pairwise comparison).
Four RCTs were identified as suitable for inclusion in the base-case network analysis (Supplementary Figure 1).7, 11, 12, 18 Data with the longest available median follow-up were utilized: CLL14, 76.4 months; GLOW, 57 months; FLAIR, 43.7 months; CLL13, 50.7 months.9, 12, 19, 20
Supplementary Table 1 provides the main clinical and biological characteristics of patients enrolled in these trials. CLL13 and FLAIR recruited younger and fitter patients, whereas CLL14 and GLOW enrolled elderly and less fit individuals.7, 11, 12, 18 However, upon stratification of the data by patient age and fitness, some heterogeneity across the trials was observed. This heterogeneity was primarily attributable to a higher proportion of patients with a Cumulative Illness Rating Scale (CIRS) score greater than 6 in the CLL14 trial compared with the GLOW trial (p = .0004). Additionally, there was a higher prevalence of patients with unmutated immunoglobulin heavy-chain variable region (IGHV) gene in the CLL13 trial compared with the FLAIR trial (p = .03) (Supplementary Table 1).
The trial analysis group consisted of 1.632 patients, with 819 (50.1%) receiving FD treatment with targeted agents and 813 (49.8%) receiving chemoimmunotherapy (CIT). Targeted agent arms evaluated VI combination in 366 (44.6%) cases (from the GLOW and FLAIR trials), and VO combination in 453 (55.3%) cases (from the CLL14 and CLL13 trials). The control arms of the RCTs employed CIT with varying intensities, reflecting differences in patient age and fitness status. Specifically, the control arms for the CLL14 and GLOW trials consisted of chlorambucil and obinutuzumab in 321 (39.4%) cases. Meanwhile, 492 (60.5%) younger and fit patients received fludarabine, cyclophosphamide, and rituximab (FCR) in the control arms of the CLL13 and FLAIR trials. Notably, of 229 patients in the CIT control arm of the CLL13 trial, 79 (34.5%) received bendamustine and rituximab (BR). However, the results of the CLL13 trial were presented in aggregate form, thereby precluding separate analysis of patients treated with BR.18
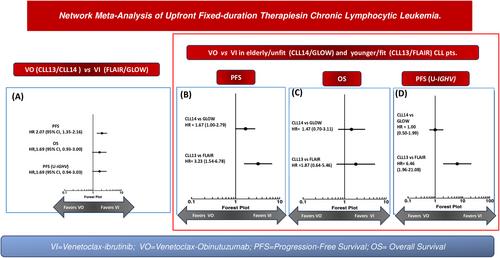
We initially analyzed the survival outcomes of patients pooled into two therapeutic groups irrespective of age and fitness status: VI (including GLOW and FLAIR studies) and VO (encompassing CLL13 and CLL14 studies). The HR values (HR 2.07; 95% CI, 1.35–2.16) suggest a twofold shorter PFS among patients treated with VO compared with those treated with VI (Figure 1A). In contrast, OS analysis did not reveal any statistically significant difference between the two venetoclax-based FD therapy groups (HR 1.69; 95% CI, 0.93–3.00) (Figure 1A).
To account for variability in the inclusion criteria across trials, particularly regarding age and comorbidities, the NMA was repeated with a focus upon trials that either recruited elderly or younger patients with CLL. Among younger, fitter patients enrolled in CLL13 and FLAIR trials, there was a significant worsening in PFS with the VO combination compared with VI (HR = 3.23, 95% CI: 1.54–6.78) (Figure 1B). However, in trials predominantly involving elderly or unfit patients (CLL14 and GLOW), PFS analysis failed to demonstrated statistical significance (HR = 1.67; 95% CI: 1.00–2.79) between VI and VO regimens (Figure 1B). Nonetheless, a favorable trend towards VI was apparent as the 95% CI for the HR approached but did not cross 1.00. Finally, in the OS analysis, both VI and VO equally impacted OS in younger/fit (HR = 1.87; 95% CI, 0.64–5.46) and elderly/unfit (HR = 1.47; 95% CI, 0.70–3.11) patients with CLL (Figure 1C).
Next, we investigated whether VI could exert a differential impact on PFS among unmutated IGHV CLL patients. Pooling together younger and elderly CLL patients, our analysis did not reveal any PFS advantage associated with the VI combination compared with VO (HR = 1.69; 95% CI, 0.94–3.03) (Figure 1A). Subsequently, in an age- and fitness-controlled analysis, younger patients (from the FLAIR and CLL13 trials) demonstrated a substantial PFS benefit with VI (HR = 6.46; 95% CI: 1.96–21.08), whereas elderly patients (from the GLOW and CLL14 trials) did not sustain this benefit (HR = 1.00; 95% CI: 0.50–1.99) (Figure 1D).
The results of this NMA definitely demonstrate improved PFS with VI compared to VO in all CLL patients, regardless of age and fitness status. This improvement is notably more pronounced among younger and fitter patients. The unique design of the FLAIR trial, involving younger/fit patients, may have influenced these findings. In this trial the duration of VI therapy depended on measurable residual disease (MRD) assessment in peripheral blood and bone marrow, potentially resulting in prolonged treatment exposure. Consequently, a significant proportion of patients discontinued VI therapy by 2 years (28.9%) and 3 years (58.0%) in the FLAIR trial,12 contrasting with the fixed 12-month duration of VO combination therapy in patients enrolled in the CLL13 trial.18
An anchored matching-adjusted indirect comparison (MAIC), presented at the 2024 European Hematological Association (EHA) meeting, evaluated the comparative efficacy of VI versus VO in elderly, medically unfit patients, from the GLOW and CLL14 trials.21 This analysis revealed that VI consistently improved all relative treatment effects, including PFS, OS, and time to next treatment (TTNT), compared with VO. Although such an analysis confirms the PFS improvement we have observed with VI in elderly and unfit CLL patients, discrepancies in methodologies used (MAIC vs. NMA) may partly account for the superior OS benefits seen with VI exclusively in the study by López-Jiménez et al.21 Nevertheless, despite the efficacy indications furnished by these indirect comparative analyses, the decision-making process for selecting the type of FD regimens in elderly, medically unfit, CLL patients must encompass factors such as renal or cardiovascular comorbidities, the perceived risk of tumor lysis syndrome (TLS), potential drug interactions, logistical considerations pertaining to the administration of parenteral therapies, and notably, patient preferences.22
We acknowledge several limitations in our data, including the limited number of studies available and the heterogeneity among patients enrolled in the RCTs used for the NMA. These factors, coupled with the absence of direct comparison data, contribute to the “moderate” level of evidence assigned by GRADE to our NMA.17 However, as we await the results of CLL17, which will address the question of FD regimen selection within an RCT, our analyses, though provisional, may offer valuable insights for clinical practice. Furthermore, ongoing Phase 3 studies such as MAJIC (NCT05057494) and CLL18 (anticipated to commence by the end of 2024), comparing VO with alternative venetoclax-based combinations involving second-generation covalent BTK inhibitors (e.g., acalabrutinib) or non-covalent BTK inhibitors (e.g., pirtobrutinib), will contribute to identifying the most effective FD regimen in CLL.
Stefano Molica designed the study, selected and evaluated studies, performed data extraction, evaluated and interpreted results, and wrote the manuscript. David Allsup interpreted results, supported with his advice the preparation of the manuscript, and wrote the paper. Diana Giannarelli selected and evaluated studies, performed data extraction, performed statistical analyses, and evaluated the results. All authors reviewed and approved the manuscript.
SM received honoraria from Janssen, Abbvie, and AstraZeneca. DA and DG declare no competing financial interests.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
