Noémie Reinert, Katinka Wetzel, Fabian Franzeck, Mario Morgenstern, Markus Aschwanden, Thomas Wolff, Martin Clauss, Parham Sendi
{"title":"糖尿病足感染管理中抗生素管理原则与实践的一致性如何:一项院内质量控制研究。","authors":"Noémie Reinert, Katinka Wetzel, Fabian Franzeck, Mario Morgenstern, Markus Aschwanden, Thomas Wolff, Martin Clauss, Parham Sendi","doi":"10.5194/jbji-9-183-2024","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b>: Standardization of diagnostic and treatment concepts in diabetes-related foot infection (DFI) is challenging. In 2019, specific recommendations regarding diagnostic principles and antibiotic therapy (ABT) for DFI, including the one for osteomyelitis (DFO), were introduced in our institution. In this study, we assessed the adherence to these in-house guidelines 2 years after their implementation. <b>Methods</b>: Adult patients with DFI with and without DFO who underwent surgical intervention between 2019 and 2021 were included. Patients' charts were retrospectively reviewed. Accordance to recommendations regarding biopsy sampling, labeling, requesting microbiological and histopathological examinations, and treatment duration were assessed. <b>Results</b>: A total of 80 patients with 117 hospital episodes and 163 surgical interventions were included; 84.6 % required an amputation. Patients with HbA1c levels of <math><mrow><mo><</mo> <mn>6.5</mn></mrow> </math> % more often required a revision during the same hospitalization than those with HbA1c levels of <math><mrow><mo>≥</mo> <mn>6.5</mn></mrow> </math> % (29.4 % vs. 12.1 %, respectively, <math><mrow><mi>p</mi> <mo>=</mo> <mn>0.023</mn></mrow> </math> ). Specimens were obtained in 71.8 % of operations and sent for histological examination in 63.2 %. The mean duration of ABT was 9 (interquartile range (IQR) 5-15) d in macroscopically surgically cured episodes and 40.5 (IQR 15-42) d in cases with resection margins in non-healthy bone ( <math><mrow><mi>p</mi> <mo><</mo> <mn>0.0001</mn></mrow> </math> ). Treatment duration results were similar when using histological results: 13 (IQR 8-42) d for healthy bone vs. 29 (IQR 13-42) d for resection margins consistent with osteomyelitis ( <math><mrow><mi>p</mi> <mo>=</mo> <mn>0.026</mn></mrow> </math> ). <b>Conclusion</b>: The adherence to recommendations in terms of biopsy sampling was good, moderate for histopathological analysis and poor for labeling the anatomic location. Adherence to recommendations for ABT duration was good, but further shortening of treatment duration for surgically cured cases is necessary.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"9 3","pages":"183-190"},"PeriodicalIF":2.8000,"publicationDate":"2024-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11262018/pdf/","citationCount":"0","resultStr":"{\"title\":\"What is the agreement between principles and practice of antibiotic stewardship in the management of diabetic foot infection: an in-hospital quality control study.\",\"authors\":\"Noémie Reinert, Katinka Wetzel, Fabian Franzeck, Mario Morgenstern, Markus Aschwanden, Thomas Wolff, Martin Clauss, Parham Sendi\",\"doi\":\"10.5194/jbji-9-183-2024\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b>: Standardization of diagnostic and treatment concepts in diabetes-related foot infection (DFI) is challenging. In 2019, specific recommendations regarding diagnostic principles and antibiotic therapy (ABT) for DFI, including the one for osteomyelitis (DFO), were introduced in our institution. In this study, we assessed the adherence to these in-house guidelines 2 years after their implementation. <b>Methods</b>: Adult patients with DFI with and without DFO who underwent surgical intervention between 2019 and 2021 were included. Patients' charts were retrospectively reviewed. Accordance to recommendations regarding biopsy sampling, labeling, requesting microbiological and histopathological examinations, and treatment duration were assessed. <b>Results</b>: A total of 80 patients with 117 hospital episodes and 163 surgical interventions were included; 84.6 % required an amputation. Patients with HbA1c levels of <math><mrow><mo><</mo> <mn>6.5</mn></mrow> </math> % more often required a revision during the same hospitalization than those with HbA1c levels of <math><mrow><mo>≥</mo> <mn>6.5</mn></mrow> </math> % (29.4 % vs. 12.1 %, respectively, <math><mrow><mi>p</mi> <mo>=</mo> <mn>0.023</mn></mrow> </math> ). Specimens were obtained in 71.8 % of operations and sent for histological examination in 63.2 %. The mean duration of ABT was 9 (interquartile range (IQR) 5-15) d in macroscopically surgically cured episodes and 40.5 (IQR 15-42) d in cases with resection margins in non-healthy bone ( <math><mrow><mi>p</mi> <mo><</mo> <mn>0.0001</mn></mrow> </math> ). Treatment duration results were similar when using histological results: 13 (IQR 8-42) d for healthy bone vs. 29 (IQR 13-42) d for resection margins consistent with osteomyelitis ( <math><mrow><mi>p</mi> <mo>=</mo> <mn>0.026</mn></mrow> </math> ). <b>Conclusion</b>: The adherence to recommendations in terms of biopsy sampling was good, moderate for histopathological analysis and poor for labeling the anatomic location. Adherence to recommendations for ABT duration was good, but further shortening of treatment duration for surgically cured cases is necessary.</p>\",\"PeriodicalId\":15271,\"journal\":{\"name\":\"Journal of Bone and Joint Infection\",\"volume\":\"9 3\",\"pages\":\"183-190\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-06-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11262018/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Bone and Joint Infection\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5194/jbji-9-183-2024\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-9-183-2024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
What is the agreement between principles and practice of antibiotic stewardship in the management of diabetic foot infection: an in-hospital quality control study.
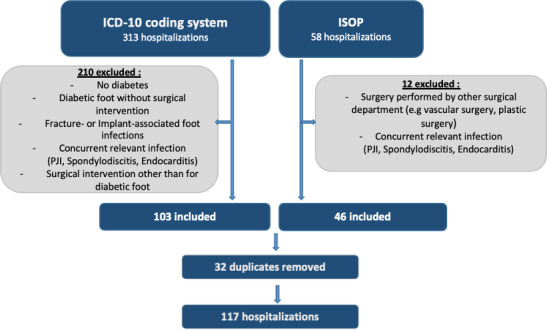
Introduction: Standardization of diagnostic and treatment concepts in diabetes-related foot infection (DFI) is challenging. In 2019, specific recommendations regarding diagnostic principles and antibiotic therapy (ABT) for DFI, including the one for osteomyelitis (DFO), were introduced in our institution. In this study, we assessed the adherence to these in-house guidelines 2 years after their implementation. Methods: Adult patients with DFI with and without DFO who underwent surgical intervention between 2019 and 2021 were included. Patients' charts were retrospectively reviewed. Accordance to recommendations regarding biopsy sampling, labeling, requesting microbiological and histopathological examinations, and treatment duration were assessed. Results: A total of 80 patients with 117 hospital episodes and 163 surgical interventions were included; 84.6 % required an amputation. Patients with HbA1c levels of % more often required a revision during the same hospitalization than those with HbA1c levels of % (29.4 % vs. 12.1 %, respectively, ). Specimens were obtained in 71.8 % of operations and sent for histological examination in 63.2 %. The mean duration of ABT was 9 (interquartile range (IQR) 5-15) d in macroscopically surgically cured episodes and 40.5 (IQR 15-42) d in cases with resection margins in non-healthy bone ( ). Treatment duration results were similar when using histological results: 13 (IQR 8-42) d for healthy bone vs. 29 (IQR 13-42) d for resection margins consistent with osteomyelitis ( ). Conclusion: The adherence to recommendations in terms of biopsy sampling was good, moderate for histopathological analysis and poor for labeling the anatomic location. Adherence to recommendations for ABT duration was good, but further shortening of treatment duration for surgically cured cases is necessary.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
