Rupam Ruchi, Elizabeth A Di Valerio, Shahab Bozorgmehri, Michael Waseer Bacchus, Benjamin K Canales, Russell Terry, John Michael DiBianco, Vincent G Bird
{"title":"药物疗法和结石矿物亚型对钙结石患者长期复发率的影响","authors":"Rupam Ruchi, Elizabeth A Di Valerio, Shahab Bozorgmehri, Michael Waseer Bacchus, Benjamin K Canales, Russell Terry, John Michael DiBianco, Vincent G Bird","doi":"10.34067/KID.0000000000000526","DOIUrl":null,"url":null,"abstract":"","PeriodicalId":17882,"journal":{"name":"Kidney360","volume":" ","pages":"1333-1340"},"PeriodicalIF":3.0000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11441814/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pharmacotherapy and Stone Mineral Subtype Influence Long-Term Recurrence Rates in Calcium Stone Formers.\",\"authors\":\"Rupam Ruchi, Elizabeth A Di Valerio, Shahab Bozorgmehri, Michael Waseer Bacchus, Benjamin K Canales, Russell Terry, John Michael DiBianco, Vincent G Bird\",\"doi\":\"10.34067/KID.0000000000000526\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"\",\"PeriodicalId\":17882,\"journal\":{\"name\":\"Kidney360\",\"volume\":\" \",\"pages\":\"1333-1340\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11441814/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kidney360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.34067/KID.0000000000000526\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34067/KID.0000000000000526","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/25 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
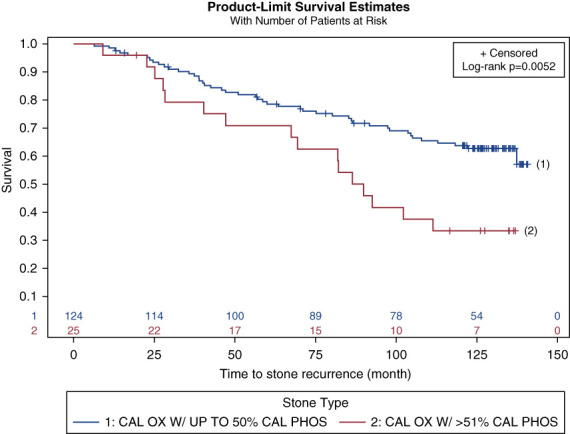
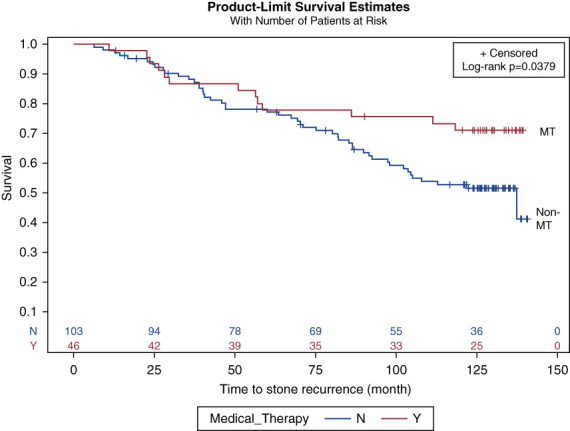
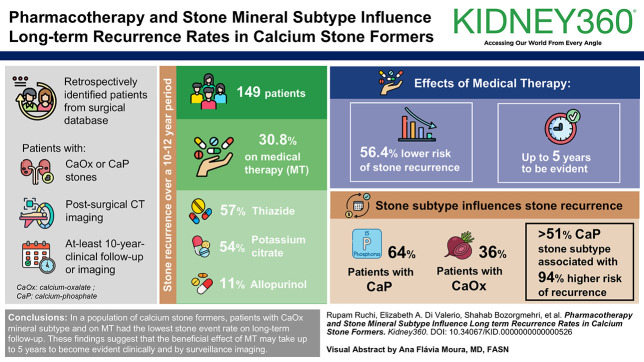
背景:肾结石的长期复发数据十分有限。我们调查了草酸钙(CaOx)和磷酸钙(CaP)结石患者在10-12年随访期间的结石复发情况:方法:我们从外科数据库中回顾性地识别了以下患者:1)CaOx 或 CaP 结石;2)手术后计算机断层扫描成像;3)至少 10 年的临床随访和成像。此外,还收集了接受噻嗪类/噻嗪类利尿剂、枸橼酸钾和/或别嘌醇等药物治疗(MT)的数据。对患者在10-12年期间的结石复发记录进行了审查。采用卡普兰-梅耶生存曲线和考克斯比例危险模型分析了结石类型、药物治疗和复发时间之间的关系。多变量分析采用 Cox 比例危险模型进行:在符合纳入标准的 149 人中,87 人(58.3%)接受了基线 24 小时尿检,46 人(30.8%)服用了噻嗪类(26/46;57%)、枸橼酸钾(25/46;54%)和别嘌呤醇(5/46;11%)等 MT 药物。与未服用噻嗪类药物的患者相比,服用噻嗪类药物的患者更有可能确诊为高血压(P=0.008),基线时也更有可能出现低胰岛素血症(P=0.01)。在平均 10.6 年的时间里,与未服用 MT 的患者相比,服用 MT 的患者发生结石的几率明显降低(21.3% vs 37.5%,p=0.04),其中有 8 人(17%)在研究期间停止服用 MT。以 CaP 矿物质亚型为主的患者比 CaOx 患者发生的结石事件更多(64% vs 36%,p=0.006),这一现象可能是由于基线尿 pH 值较高(>6,58.8% vs 33.9%,p=0.02)所致。通过生存分析,结石亚型和MT的影响分别在随访第20个月和第60个月时变得明显:结论:在高复发风险的钙结石患者中,CaOx矿物亚型和MT患者在长期随访中的结石发生率最低。这些研究结果表明,药物治疗的有益效果可能需要长达 5 年的时间才能在临床和监测成像中显现出来。




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
