Georg Semmler , Lorenz Balcar , Benedikt Simbrunner , Lukas Hartl , Mathias Jachs , Michael Schwarz , Benedikt Silvester Hofer , Laurenz Fritz , Anna Schedlbauer , Katharina Stopfer , Daniela Neumayer , Jurij Maurer , Sophie Gensluckner , Bernhard Scheiner , Elmar Aigner , Michael Trauner , Thomas Reiberger , Mattias Mandorfer
{"title":"三级医疗机构肝脏风险评分的诊断和预后性能","authors":"Georg Semmler , Lorenz Balcar , Benedikt Simbrunner , Lukas Hartl , Mathias Jachs , Michael Schwarz , Benedikt Silvester Hofer , Laurenz Fritz , Anna Schedlbauer , Katharina Stopfer , Daniela Neumayer , Jurij Maurer , Sophie Gensluckner , Bernhard Scheiner , Elmar Aigner , Michael Trauner , Thomas Reiberger , Mattias Mandorfer","doi":"10.1016/j.jhepr.2024.101169","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><div>The LiverRisk score has been proposed as a blood-based tool to estimate liver stiffness measurement (LSM), thereby stratifying the risk of compensated advanced chronic liver disease (cACLD, LSM ≥10 kPa) and liver-related events in patients without known chronic liver disease (CLD). We aimed to evaluate its diagnostic/prognostic performance in tertiary care.</div></div><div><h3>Methods</h3><div>Patients referred to two hepatology outpatient clinics (cohort I, n = 5,897; cohort II, n = 1,558) were retrospectively included. Calibration/agreement of the LiverRisk score with LSM was assessed, and diagnostic accuracy for cACLD was compared with that of fibrosis-4 (FIB-4)/aspartate aminotransferase-to-platelet ratio index (APRI). The prediction of hepatic decompensation and utility of proposed cut-offs were evaluated.</div></div><div><h3>Results</h3><div>In cohort I/II, mean age was 48.3/51.8 years, 44.2%/44.7% were female, predominant etiologies were viral hepatitis (51.8%)/metabolic dysfunction-associated steatotic liver disease (63.7%), median LSM was 6.9 (IQR 5.1–10.9)/5.8 (IQR 4.5–8.8) kPa, and 1,690 (28.7%)/322 (20.7%) patients had cACLD.</div><div>Despite a moderate correlation (Pearson’s r = 0.325/0.422), the LiverRisk score systematically underestimated LSM (2.93/1.80 points/kPa lower), and range of agreement was wide, especially at higher values.</div><div>The diagnostic accuracy of the LiverRisk score for cACLD (area under the receiver operator characteristics curve [AUROC] 0.757/0.790) was comparable to that of FIB-4 (AUROC 0.769/0.813) and APRI (AUROC 0.747/0.765). The proposed cut-off of 10 points yielded an accuracy of 74.2%/81.2%, high specificity (91.9%/93.4%), but low negative predictive value (76.6%/84.5%, Cohen’s κ = 0.260/0.327).</div><div>In cohort I, 208 (3.5%) patients developed hepatic decompensation (median follow-up 4.7 years). The LiverRisk score showed a reasonable accuracy for predicting hepatic decompensation within 1–5 years (AUROC 0.778–0.832). However, it was inferior to LSM (AUROC 0.847–0.901, <em>p</em> <0.001) and FIB-4 (AUROC 0.898–0.913, <em>p</em> <0.001). Similar to the strata of other non-invasive tests, the proposed LiverRisk groups had distinct risks of hepatic decompensation.</div></div><div><h3>Conclusions</h3><div>The LiverRisk score did not improve the diagnosis of cACLD or prediction of hepatic decompensation in the tertiary care setting.</div></div><div><h3>Impact and implications</h3><div>The LiverRisk score has been proposed as a non-invasive tool to estimate liver stiffness measurement and thus the risk of compensated advanced chronic liver disease and liver-related events. As automatic implementation into lab reports is being discussed, the question of its applicability outside of opportunistic screening in the general population arises. In two large cohorts of patients referred to hepatology outpatient clinics, the LiverRisk score did not accurately predict liver stiffness, did not improve cACLD identification, and had a lower predictive performance for hepatic decompensation as compared with FIB-4. Although it represents a major step forward for screening patients without known liver disease in primary care, our findings indicate that the LiverRisk score does not improve patient management outside the primary care setting, that is, in cohorts with a higher pre-test probability of cACLD.</div></div>","PeriodicalId":14764,"journal":{"name":"JHEP Reports","volume":"6 11","pages":"Article 101169"},"PeriodicalIF":8.7000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Diagnostic and prognostic performance of the LiverRisk score in tertiary care\",\"authors\":\"Georg Semmler , Lorenz Balcar , Benedikt Simbrunner , Lukas Hartl , Mathias Jachs , Michael Schwarz , Benedikt Silvester Hofer , Laurenz Fritz , Anna Schedlbauer , Katharina Stopfer , Daniela Neumayer , Jurij Maurer , Sophie Gensluckner , Bernhard Scheiner , Elmar Aigner , Michael Trauner , Thomas Reiberger , Mattias Mandorfer\",\"doi\":\"10.1016/j.jhepr.2024.101169\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background & Aims</h3><div>The LiverRisk score has been proposed as a blood-based tool to estimate liver stiffness measurement (LSM), thereby stratifying the risk of compensated advanced chronic liver disease (cACLD, LSM ≥10 kPa) and liver-related events in patients without known chronic liver disease (CLD). We aimed to evaluate its diagnostic/prognostic performance in tertiary care.</div></div><div><h3>Methods</h3><div>Patients referred to two hepatology outpatient clinics (cohort I, n = 5,897; cohort II, n = 1,558) were retrospectively included. Calibration/agreement of the LiverRisk score with LSM was assessed, and diagnostic accuracy for cACLD was compared with that of fibrosis-4 (FIB-4)/aspartate aminotransferase-to-platelet ratio index (APRI). The prediction of hepatic decompensation and utility of proposed cut-offs were evaluated.</div></div><div><h3>Results</h3><div>In cohort I/II, mean age was 48.3/51.8 years, 44.2%/44.7% were female, predominant etiologies were viral hepatitis (51.8%)/metabolic dysfunction-associated steatotic liver disease (63.7%), median LSM was 6.9 (IQR 5.1–10.9)/5.8 (IQR 4.5–8.8) kPa, and 1,690 (28.7%)/322 (20.7%) patients had cACLD.</div><div>Despite a moderate correlation (Pearson’s r = 0.325/0.422), the LiverRisk score systematically underestimated LSM (2.93/1.80 points/kPa lower), and range of agreement was wide, especially at higher values.</div><div>The diagnostic accuracy of the LiverRisk score for cACLD (area under the receiver operator characteristics curve [AUROC] 0.757/0.790) was comparable to that of FIB-4 (AUROC 0.769/0.813) and APRI (AUROC 0.747/0.765). The proposed cut-off of 10 points yielded an accuracy of 74.2%/81.2%, high specificity (91.9%/93.4%), but low negative predictive value (76.6%/84.5%, Cohen’s κ = 0.260/0.327).</div><div>In cohort I, 208 (3.5%) patients developed hepatic decompensation (median follow-up 4.7 years). The LiverRisk score showed a reasonable accuracy for predicting hepatic decompensation within 1–5 years (AUROC 0.778–0.832). However, it was inferior to LSM (AUROC 0.847–0.901, <em>p</em> <0.001) and FIB-4 (AUROC 0.898–0.913, <em>p</em> <0.001). Similar to the strata of other non-invasive tests, the proposed LiverRisk groups had distinct risks of hepatic decompensation.</div></div><div><h3>Conclusions</h3><div>The LiverRisk score did not improve the diagnosis of cACLD or prediction of hepatic decompensation in the tertiary care setting.</div></div><div><h3>Impact and implications</h3><div>The LiverRisk score has been proposed as a non-invasive tool to estimate liver stiffness measurement and thus the risk of compensated advanced chronic liver disease and liver-related events. As automatic implementation into lab reports is being discussed, the question of its applicability outside of opportunistic screening in the general population arises. In two large cohorts of patients referred to hepatology outpatient clinics, the LiverRisk score did not accurately predict liver stiffness, did not improve cACLD identification, and had a lower predictive performance for hepatic decompensation as compared with FIB-4. Although it represents a major step forward for screening patients without known liver disease in primary care, our findings indicate that the LiverRisk score does not improve patient management outside the primary care setting, that is, in cohorts with a higher pre-test probability of cACLD.</div></div>\",\"PeriodicalId\":14764,\"journal\":{\"name\":\"JHEP Reports\",\"volume\":\"6 11\",\"pages\":\"Article 101169\"},\"PeriodicalIF\":8.7000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JHEP Reports\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2589555924001733\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JHEP Reports","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589555924001733","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Diagnostic and prognostic performance of the LiverRisk score in tertiary care
Background & Aims
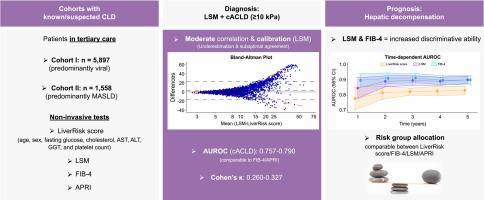
The LiverRisk score has been proposed as a blood-based tool to estimate liver stiffness measurement (LSM), thereby stratifying the risk of compensated advanced chronic liver disease (cACLD, LSM ≥10 kPa) and liver-related events in patients without known chronic liver disease (CLD). We aimed to evaluate its diagnostic/prognostic performance in tertiary care.
Methods
Patients referred to two hepatology outpatient clinics (cohort I, n = 5,897; cohort II, n = 1,558) were retrospectively included. Calibration/agreement of the LiverRisk score with LSM was assessed, and diagnostic accuracy for cACLD was compared with that of fibrosis-4 (FIB-4)/aspartate aminotransferase-to-platelet ratio index (APRI). The prediction of hepatic decompensation and utility of proposed cut-offs were evaluated.
Results
In cohort I/II, mean age was 48.3/51.8 years, 44.2%/44.7% were female, predominant etiologies were viral hepatitis (51.8%)/metabolic dysfunction-associated steatotic liver disease (63.7%), median LSM was 6.9 (IQR 5.1–10.9)/5.8 (IQR 4.5–8.8) kPa, and 1,690 (28.7%)/322 (20.7%) patients had cACLD.
Despite a moderate correlation (Pearson’s r = 0.325/0.422), the LiverRisk score systematically underestimated LSM (2.93/1.80 points/kPa lower), and range of agreement was wide, especially at higher values.
The diagnostic accuracy of the LiverRisk score for cACLD (area under the receiver operator characteristics curve [AUROC] 0.757/0.790) was comparable to that of FIB-4 (AUROC 0.769/0.813) and APRI (AUROC 0.747/0.765). The proposed cut-off of 10 points yielded an accuracy of 74.2%/81.2%, high specificity (91.9%/93.4%), but low negative predictive value (76.6%/84.5%, Cohen’s κ = 0.260/0.327).
In cohort I, 208 (3.5%) patients developed hepatic decompensation (median follow-up 4.7 years). The LiverRisk score showed a reasonable accuracy for predicting hepatic decompensation within 1–5 years (AUROC 0.778–0.832). However, it was inferior to LSM (AUROC 0.847–0.901, p <0.001) and FIB-4 (AUROC 0.898–0.913, p <0.001). Similar to the strata of other non-invasive tests, the proposed LiverRisk groups had distinct risks of hepatic decompensation.
Conclusions
The LiverRisk score did not improve the diagnosis of cACLD or prediction of hepatic decompensation in the tertiary care setting.
Impact and implications
The LiverRisk score has been proposed as a non-invasive tool to estimate liver stiffness measurement and thus the risk of compensated advanced chronic liver disease and liver-related events. As automatic implementation into lab reports is being discussed, the question of its applicability outside of opportunistic screening in the general population arises. In two large cohorts of patients referred to hepatology outpatient clinics, the LiverRisk score did not accurately predict liver stiffness, did not improve cACLD identification, and had a lower predictive performance for hepatic decompensation as compared with FIB-4. Although it represents a major step forward for screening patients without known liver disease in primary care, our findings indicate that the LiverRisk score does not improve patient management outside the primary care setting, that is, in cohorts with a higher pre-test probability of cACLD.
期刊介绍:
JHEP Reports is an open access journal that is affiliated with the European Association for the Study of the Liver (EASL). It serves as a companion journal to the highly respected Journal of Hepatology.
The primary objective of JHEP Reports is to publish original papers and reviews that contribute to the advancement of knowledge in the field of liver diseases. The journal covers a wide range of topics, including basic, translational, and clinical research. It also focuses on global issues in hepatology, with particular emphasis on areas such as clinical trials, novel diagnostics, precision medicine and therapeutics, cancer research, cellular and molecular studies, artificial intelligence, microbiome research, epidemiology, and cutting-edge technologies.
In summary, JHEP Reports is dedicated to promoting scientific discoveries and innovations in liver diseases through the publication of high-quality research papers and reviews covering various aspects of hepatology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
