Nawal Khan, Maria de la Torre, Houyar Moghaddas, Nelli Fromer, Siarhei Melnikau
{"title":"同步乳腺癌和肺癌的病例报告,三种不同的病理诊断。","authors":"Nawal Khan, Maria de la Torre, Houyar Moghaddas, Nelli Fromer, Siarhei Melnikau","doi":"10.21037/acr-23-194","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multiple primary malignant tumors (MPMTs) pose a significant clinical challenge, denoting the occurrence of two or more distinct malignant tumors with differing histological characteristics, all diagnosed within a 6-month timeframe. MPMT is a rare condition and due to the unique treatment requirements for each specific cancer type, it is crucial for healthcare professionals to accurately differentiate between metastatic growth and distinct primary tumors.</p><p><strong>Case description: </strong>In this case report, we present a 41-year-old female patient who received diagnoses of three separate synchronous primary tumors. The patient presented for evaluation of a right breast mass that had been present for 1 year. Initial diagnostic tests, including mammography and ultrasound, did not provide any conclusive results. Subsequent magnetic resonance imaging (MRI) of the breast prompted an ultrasound-guided biopsy which confirmed moderately differentiated invasive ductal carcinoma (IDC). During pre-surgical testing, a suspicious opacity was detected on a chest X-ray, prompting further investigation with a computed tomography (CT) scan of the chest to distinguish between metastatic disease and a potential new primary tumor. Clinical and pathological examinations revealed the presence of bilateral masses originating from two different origins: invasive mucinous pulmonary adenocarcinoma in the left lower lobe and a neuroendocrine carcinoma in the right middle lobe of the lung.</p><p><strong>Conclusions: </strong>Cases of this nature present a complex challenge to physicians and underscore the critical importance of maintaining a high level of clinical suspicion to ensure the delivery of high-quality care. Effective management of such patients requires a multidisciplinary collaboration among breast surgeons, thoracic surgeons, and medical and radiation oncologists.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"8 ","pages":"68"},"PeriodicalIF":0.7000,"publicationDate":"2024-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11292063/pdf/","citationCount":"0","resultStr":"{\"title\":\"A case report of synchronous breast and lung cancer with three different pathologic diagnoses.\",\"authors\":\"Nawal Khan, Maria de la Torre, Houyar Moghaddas, Nelli Fromer, Siarhei Melnikau\",\"doi\":\"10.21037/acr-23-194\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Multiple primary malignant tumors (MPMTs) pose a significant clinical challenge, denoting the occurrence of two or more distinct malignant tumors with differing histological characteristics, all diagnosed within a 6-month timeframe. MPMT is a rare condition and due to the unique treatment requirements for each specific cancer type, it is crucial for healthcare professionals to accurately differentiate between metastatic growth and distinct primary tumors.</p><p><strong>Case description: </strong>In this case report, we present a 41-year-old female patient who received diagnoses of three separate synchronous primary tumors. The patient presented for evaluation of a right breast mass that had been present for 1 year. Initial diagnostic tests, including mammography and ultrasound, did not provide any conclusive results. Subsequent magnetic resonance imaging (MRI) of the breast prompted an ultrasound-guided biopsy which confirmed moderately differentiated invasive ductal carcinoma (IDC). During pre-surgical testing, a suspicious opacity was detected on a chest X-ray, prompting further investigation with a computed tomography (CT) scan of the chest to distinguish between metastatic disease and a potential new primary tumor. Clinical and pathological examinations revealed the presence of bilateral masses originating from two different origins: invasive mucinous pulmonary adenocarcinoma in the left lower lobe and a neuroendocrine carcinoma in the right middle lobe of the lung.</p><p><strong>Conclusions: </strong>Cases of this nature present a complex challenge to physicians and underscore the critical importance of maintaining a high level of clinical suspicion to ensure the delivery of high-quality care. Effective management of such patients requires a multidisciplinary collaboration among breast surgeons, thoracic surgeons, and medical and radiation oncologists.</p>\",\"PeriodicalId\":29752,\"journal\":{\"name\":\"AME Case Reports\",\"volume\":\"8 \",\"pages\":\"68\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-06-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11292063/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AME Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/acr-23-194\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-23-194","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:多原发恶性肿瘤(MPMT)是一项重大的临床挑战,它是指在 6 个月的时间内诊断出两种或两种以上组织学特征不同的恶性肿瘤。MPMT 是一种罕见病,由于每种特定癌症类型都有独特的治疗要求,因此医护人员准确区分转移性生长和不同的原发肿瘤至关重要:在本病例报告中,我们介绍了一名 41 岁的女性患者,她被诊断出患有三个不同的同步原发肿瘤。患者因右侧乳房肿块就诊,该肿块已存在 1 年。最初的诊断检查,包括乳房 X 线照相术和超声波检查,都没有得出任何结论性结果。随后进行的乳腺磁共振成像(MRI)促使患者在超声引导下进行活检,结果证实为中度分化的浸润性导管癌(IDC)。在手术前的检查中,胸部 X 光片发现了可疑的不透明物,这促使她进一步进行胸部计算机断层扫描(CT)检查,以区分转移性疾病和潜在的新原发肿瘤。临床和病理检查显示,双侧肿块有两个不同的来源:左肺下叶的浸润性粘液性肺腺癌和右肺中叶的神经内分泌癌:这种性质的病例给医生带来了复杂的挑战,并强调了保持高度临床怀疑以确保提供高质量护理的重要性。此类患者的有效治疗需要乳腺外科医生、胸外科医生以及肿瘤内科和放射科医生的多学科合作。
A case report of synchronous breast and lung cancer with three different pathologic diagnoses.
Background: Multiple primary malignant tumors (MPMTs) pose a significant clinical challenge, denoting the occurrence of two or more distinct malignant tumors with differing histological characteristics, all diagnosed within a 6-month timeframe. MPMT is a rare condition and due to the unique treatment requirements for each specific cancer type, it is crucial for healthcare professionals to accurately differentiate between metastatic growth and distinct primary tumors.
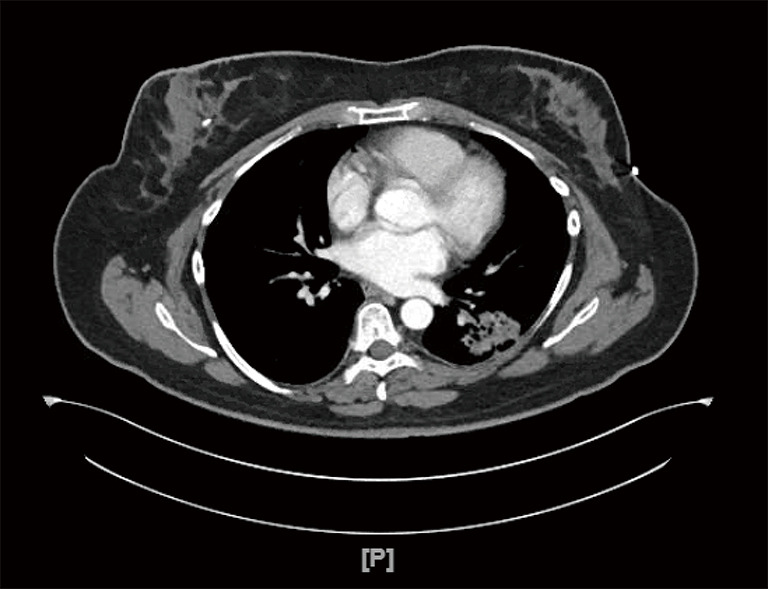
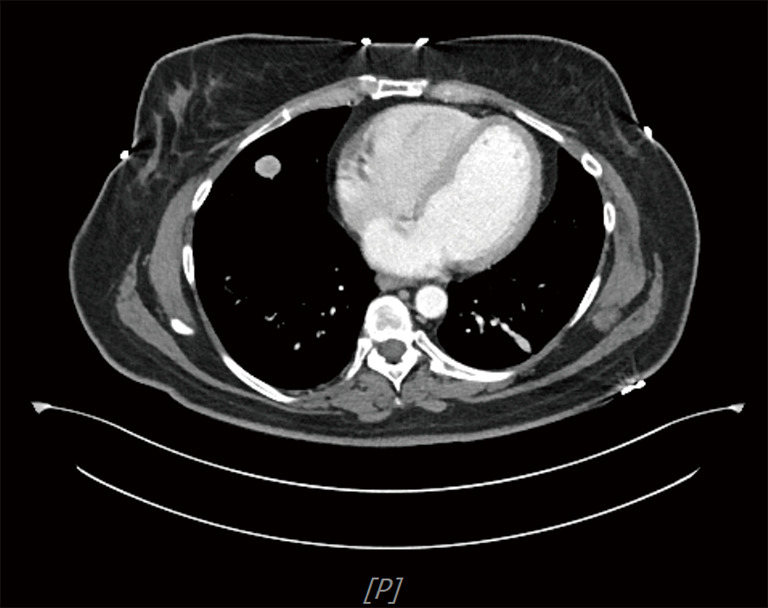
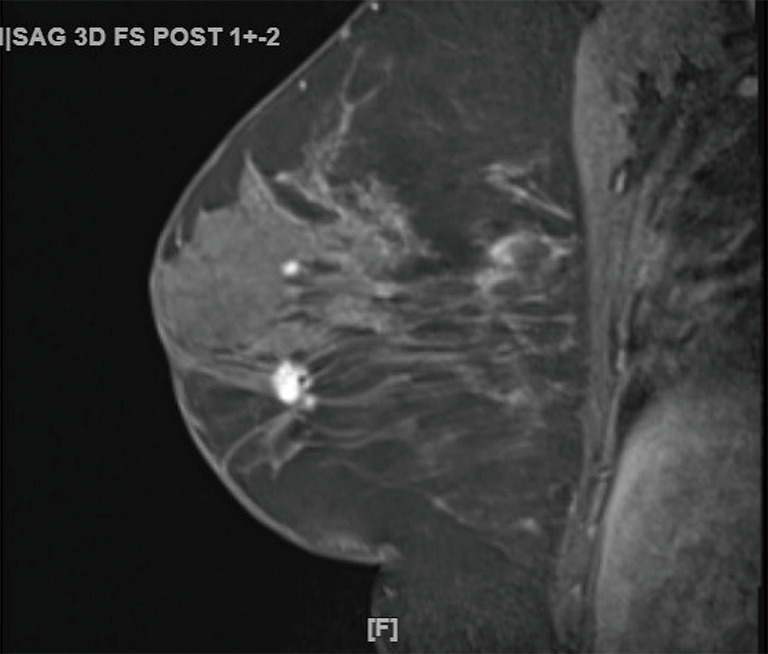
Case description: In this case report, we present a 41-year-old female patient who received diagnoses of three separate synchronous primary tumors. The patient presented for evaluation of a right breast mass that had been present for 1 year. Initial diagnostic tests, including mammography and ultrasound, did not provide any conclusive results. Subsequent magnetic resonance imaging (MRI) of the breast prompted an ultrasound-guided biopsy which confirmed moderately differentiated invasive ductal carcinoma (IDC). During pre-surgical testing, a suspicious opacity was detected on a chest X-ray, prompting further investigation with a computed tomography (CT) scan of the chest to distinguish between metastatic disease and a potential new primary tumor. Clinical and pathological examinations revealed the presence of bilateral masses originating from two different origins: invasive mucinous pulmonary adenocarcinoma in the left lower lobe and a neuroendocrine carcinoma in the right middle lobe of the lung.
Conclusions: Cases of this nature present a complex challenge to physicians and underscore the critical importance of maintaining a high level of clinical suspicion to ensure the delivery of high-quality care. Effective management of such patients requires a multidisciplinary collaboration among breast surgeons, thoracic surgeons, and medical and radiation oncologists.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
