{"title":"直肠癌患者癌症特异性死亡率的最新种族/族裔差异。","authors":"Lu Li, Zhenpeng Xu, Guanghua Chen, Leichang Zhang, Zhihua Lu, Chen Chen, Yugen Chen","doi":"10.21037/tgh-24-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>African American patients frequently receive nonstandard treatment and demonstrate poorer overall survival (OS) outcomes compared to White patients. Our objective was to analysis whether racial/ethnic disparities in rectal cancer-specific mortality remain after accounting for clinical characteristics, treatment, and access-to-care-related factors.</p><p><strong>Methods: </strong>Individuals diagnosed with rectal cancer between 2011 and 2020 were identified using the Surveillance, Epidemiology, and End Results Database. The cumulative incidence of rectal cancer-specific mortality was computed. Sub-distribution hazard ratios (sdHRs) and 95% confidence intervals (CIs) for rectal cancer-specific mortality associated with race/ethnicity were estimated using Fine and Gray model with stepwise adjustments for clinical characteristics, treatment modalities, and factors related to access-to-care.</p><p><strong>Results: </strong>Among 54,370 patients, non-Hispanic (NH) Black individuals exhibited the highest cumulative incidence of rectal cancer-specific mortality (39%), followed by American Indian/Alaska Native (AI/AN) (35%), Hispanics (32%), NH-White (31%), and Asian/Pacific Islander (API) (30%). After adjusting for clinical characteristics, NH-Black patients had a 28% increased risk of rectal cancer mortality (sdHR, 1.28; 95% CI: 1.20-1.35) compared to NH-White patients. In contrast, mortality disparities between Hispanic-White, AI/AN-White, and API-White groups were not significant. The Black-White mortality differences persisted even after adjustments for treatment and access-to-care-related factors. In stratified analyses, among patients with a median household income below $59,999, AI/AN patients showed higher mortality than NH-Whites when adjusted for clinical characteristics (sdHR, 1.32; 95% CI: 1.03-1.70).</p><p><strong>Conclusions: </strong>Overall, the racial/ethnic disparities in rectal cancer-specific mortality were largely attributable to differences in clinical characteristics, treatment modalities, and factors related to access-to-care. These findings emphasize the critical need for equitable healthcare to effectively address and reduce the significant racial/ethnic disparities in rectal cancer outcomes.</p>","PeriodicalId":94362,"journal":{"name":"Translational gastroenterology and hepatology","volume":"9 ","pages":"37"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11292083/pdf/","citationCount":"0","resultStr":"{\"title\":\"Recent racial/ethnic disparities in cancer-specific mortality among patients diagnosed with rectal cancer.\",\"authors\":\"Lu Li, Zhenpeng Xu, Guanghua Chen, Leichang Zhang, Zhihua Lu, Chen Chen, Yugen Chen\",\"doi\":\"10.21037/tgh-24-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>African American patients frequently receive nonstandard treatment and demonstrate poorer overall survival (OS) outcomes compared to White patients. Our objective was to analysis whether racial/ethnic disparities in rectal cancer-specific mortality remain after accounting for clinical characteristics, treatment, and access-to-care-related factors.</p><p><strong>Methods: </strong>Individuals diagnosed with rectal cancer between 2011 and 2020 were identified using the Surveillance, Epidemiology, and End Results Database. The cumulative incidence of rectal cancer-specific mortality was computed. Sub-distribution hazard ratios (sdHRs) and 95% confidence intervals (CIs) for rectal cancer-specific mortality associated with race/ethnicity were estimated using Fine and Gray model with stepwise adjustments for clinical characteristics, treatment modalities, and factors related to access-to-care.</p><p><strong>Results: </strong>Among 54,370 patients, non-Hispanic (NH) Black individuals exhibited the highest cumulative incidence of rectal cancer-specific mortality (39%), followed by American Indian/Alaska Native (AI/AN) (35%), Hispanics (32%), NH-White (31%), and Asian/Pacific Islander (API) (30%). After adjusting for clinical characteristics, NH-Black patients had a 28% increased risk of rectal cancer mortality (sdHR, 1.28; 95% CI: 1.20-1.35) compared to NH-White patients. In contrast, mortality disparities between Hispanic-White, AI/AN-White, and API-White groups were not significant. The Black-White mortality differences persisted even after adjustments for treatment and access-to-care-related factors. In stratified analyses, among patients with a median household income below $59,999, AI/AN patients showed higher mortality than NH-Whites when adjusted for clinical characteristics (sdHR, 1.32; 95% CI: 1.03-1.70).</p><p><strong>Conclusions: </strong>Overall, the racial/ethnic disparities in rectal cancer-specific mortality were largely attributable to differences in clinical characteristics, treatment modalities, and factors related to access-to-care. These findings emphasize the critical need for equitable healthcare to effectively address and reduce the significant racial/ethnic disparities in rectal cancer outcomes.</p>\",\"PeriodicalId\":94362,\"journal\":{\"name\":\"Translational gastroenterology and hepatology\",\"volume\":\"9 \",\"pages\":\"37\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-06-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11292083/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational gastroenterology and hepatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/tgh-24-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/tgh-24-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:非裔美国人患者经常接受非标准治疗,与白人患者相比,他们的总生存率(OS)较低。我们的目的是分析在考虑临床特征、治疗和获得护理相关因素后,直肠癌特异性死亡率的种族/民族差异是否仍然存在:方法:我们使用监测、流行病学和最终结果数据库对 2011 年至 2020 年间确诊为直肠癌的患者进行了鉴定。计算直肠癌特异性死亡率的累积发病率。使用 Fine and Gray 模型估算了与种族/民族相关的直肠癌特异性死亡率的子分布危险比 (sdHRs) 和 95% 置信区间 (CIs),并逐步调整了临床特征、治疗方式和获得护理的相关因素:在54,370名患者中,非西班牙裔(NH)黑人的直肠癌特异性死亡率累积发生率最高(39%),其次是美洲印第安人/阿拉斯加原住民(AI/AN)(35%)、西班牙裔(32%)、NH-白人(31%)和亚洲/太平洋岛民(API)(30%)。调整临床特征后,与新罕布什尔-白人患者相比,新罕布什尔-黑人患者的直肠癌死亡风险增加了 28%(sdHR,1.28;95% CI:1.20-1.35)。相比之下,西班牙裔白人、亚裔美国人/印第安人-白人和亚裔美国人-白人群体之间的死亡率差异并不显著。即使对治疗和获得护理的相关因素进行调整后,黑人与白人的死亡率差异依然存在。在分层分析中,在家庭收入中位数低于 59999 美元的患者中,根据临床特征进行调整后,亚裔美国人/印第安人患者的死亡率高于新罕布什尔白人(sdHR,1.32;95% CI:1.03-1.70):总体而言,直肠癌特异性死亡率的种族/民族差异主要归因于临床特征、治疗方式和获得护理相关因素的差异。这些发现强调了公平医疗保健的重要性,以有效解决和减少直肠癌治疗结果中的种族/民族差异。
Recent racial/ethnic disparities in cancer-specific mortality among patients diagnosed with rectal cancer.
Background: African American patients frequently receive nonstandard treatment and demonstrate poorer overall survival (OS) outcomes compared to White patients. Our objective was to analysis whether racial/ethnic disparities in rectal cancer-specific mortality remain after accounting for clinical characteristics, treatment, and access-to-care-related factors.
Methods: Individuals diagnosed with rectal cancer between 2011 and 2020 were identified using the Surveillance, Epidemiology, and End Results Database. The cumulative incidence of rectal cancer-specific mortality was computed. Sub-distribution hazard ratios (sdHRs) and 95% confidence intervals (CIs) for rectal cancer-specific mortality associated with race/ethnicity were estimated using Fine and Gray model with stepwise adjustments for clinical characteristics, treatment modalities, and factors related to access-to-care.
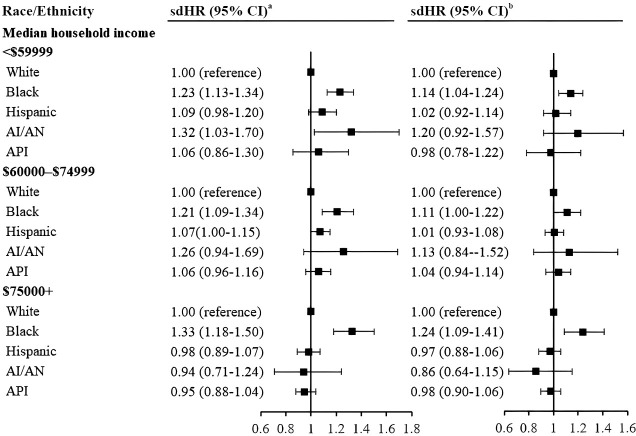
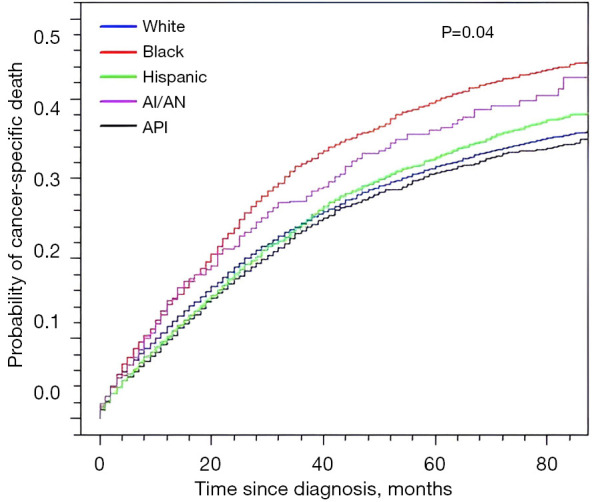
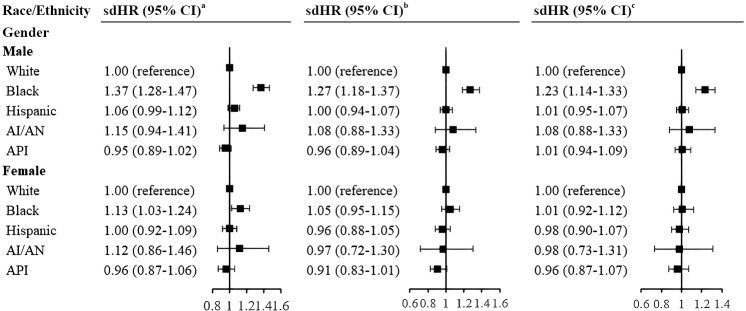
Results: Among 54,370 patients, non-Hispanic (NH) Black individuals exhibited the highest cumulative incidence of rectal cancer-specific mortality (39%), followed by American Indian/Alaska Native (AI/AN) (35%), Hispanics (32%), NH-White (31%), and Asian/Pacific Islander (API) (30%). After adjusting for clinical characteristics, NH-Black patients had a 28% increased risk of rectal cancer mortality (sdHR, 1.28; 95% CI: 1.20-1.35) compared to NH-White patients. In contrast, mortality disparities between Hispanic-White, AI/AN-White, and API-White groups were not significant. The Black-White mortality differences persisted even after adjustments for treatment and access-to-care-related factors. In stratified analyses, among patients with a median household income below $59,999, AI/AN patients showed higher mortality than NH-Whites when adjusted for clinical characteristics (sdHR, 1.32; 95% CI: 1.03-1.70).
Conclusions: Overall, the racial/ethnic disparities in rectal cancer-specific mortality were largely attributable to differences in clinical characteristics, treatment modalities, and factors related to access-to-care. These findings emphasize the critical need for equitable healthcare to effectively address and reduce the significant racial/ethnic disparities in rectal cancer outcomes.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
