Charlène J van der Zijden, Pim B Olthof, Pieter C van der Sluis, Bas P L Wijnhoven, Maria Erodotou, Henk H Hartgrink, Boudewijn van Etten, Stijn van Esser, Sjoerd M Lagarde, Jan Willem T Dekker
{"title":"食管癌中的 N3 疾病:来自全国登记处的结果。","authors":"Charlène J van der Zijden, Pim B Olthof, Pieter C van der Sluis, Bas P L Wijnhoven, Maria Erodotou, Henk H Hartgrink, Boudewijn van Etten, Stijn van Esser, Sjoerd M Lagarde, Jan Willem T Dekker","doi":"10.1159/000540468","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with extensive lymph node metastases have a poor prognosis. Clinical staging of lymph node metastases poses significant challenges given the limited sensitivity and specificity of imaging techniques. The aim of this study was to investigate the overall survival (OS) of patients with N3 disease in a real-world Dutch population and the added value of surgery in these patients.</p><p><strong>Methods: </strong>Patients with cN3M0 esophageal or gastroesophageal cancer were identified from the Netherlands Cancer Registry (2012-2019). Treatment consisted of neoadjuvant chemo(radio)therapy followed by resection or chemo(radio)therapy, radiotherapy, or esophagectomy alone. OS was calculated using the Kaplan-Meier method.</p><p><strong>Results: </strong>Some 21,566 patients were diagnosed with esophageal cancer of whom 359 (1.7%) had cN3M0 disease. Median OS of these patients was 12.5 months (95% CI: 10.7-14.3). Median OS following chemoradiotherapy alone and neoadjuvant therapy plus surgery was 13.3 months (95% CI: 10.7-15.9) and 23.7 months (95% CI: 18.3-29.2), respectively. Of all patients who underwent esophagectomy, 391 (2.8%) had (y)pN3 disease, and median OS was 16.1 months (95% CI: 14.8-17.4). Twenty-one patients (5.4%) were correctly classified as cN3, and 3-year OS was 21%.</p><p><strong>Conclusion(s): </strong>Clinical staging appears to be difficult, apparently in patients with N3 esophageal cancer. Surgery seems to be of benefit to these patients. More research is required to address the ongoing challenges in clinical staging and the best neoadjuvant therapy.</p>","PeriodicalId":11241,"journal":{"name":"Digestive Surgery","volume":" ","pages":"133-140"},"PeriodicalIF":1.2000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11382634/pdf/","citationCount":"0","resultStr":"{\"title\":\"N3 Disease in Esophageal Cancer: Results from a Nationwide Registry.\",\"authors\":\"Charlène J van der Zijden, Pim B Olthof, Pieter C van der Sluis, Bas P L Wijnhoven, Maria Erodotou, Henk H Hartgrink, Boudewijn van Etten, Stijn van Esser, Sjoerd M Lagarde, Jan Willem T Dekker\",\"doi\":\"10.1159/000540468\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with extensive lymph node metastases have a poor prognosis. Clinical staging of lymph node metastases poses significant challenges given the limited sensitivity and specificity of imaging techniques. The aim of this study was to investigate the overall survival (OS) of patients with N3 disease in a real-world Dutch population and the added value of surgery in these patients.</p><p><strong>Methods: </strong>Patients with cN3M0 esophageal or gastroesophageal cancer were identified from the Netherlands Cancer Registry (2012-2019). Treatment consisted of neoadjuvant chemo(radio)therapy followed by resection or chemo(radio)therapy, radiotherapy, or esophagectomy alone. OS was calculated using the Kaplan-Meier method.</p><p><strong>Results: </strong>Some 21,566 patients were diagnosed with esophageal cancer of whom 359 (1.7%) had cN3M0 disease. Median OS of these patients was 12.5 months (95% CI: 10.7-14.3). Median OS following chemoradiotherapy alone and neoadjuvant therapy plus surgery was 13.3 months (95% CI: 10.7-15.9) and 23.7 months (95% CI: 18.3-29.2), respectively. Of all patients who underwent esophagectomy, 391 (2.8%) had (y)pN3 disease, and median OS was 16.1 months (95% CI: 14.8-17.4). Twenty-one patients (5.4%) were correctly classified as cN3, and 3-year OS was 21%.</p><p><strong>Conclusion(s): </strong>Clinical staging appears to be difficult, apparently in patients with N3 esophageal cancer. Surgery seems to be of benefit to these patients. More research is required to address the ongoing challenges in clinical staging and the best neoadjuvant therapy.</p>\",\"PeriodicalId\":11241,\"journal\":{\"name\":\"Digestive Surgery\",\"volume\":\" \",\"pages\":\"133-140\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11382634/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000540468\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000540468","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:有广泛淋巴结转移的患者预后较差。由于成像技术的敏感性和特异性有限,淋巴结转移的临床分期面临巨大挑战。本研究旨在调查荷兰真实人群中 N3 疾病患者的总生存率(OS)以及手术对这些患者的附加价值:方法:从荷兰癌症登记处(2012-2019年)中确定了cN3M0食管癌或胃食管癌患者。治疗方法包括新辅助化疗(放疗)、切除术或化疗(放疗)、放疗或单纯食管切除术。采用Kaplan-Meier法计算OS:结果:约 21 566 名食管癌患者被确诊为食管癌,其中 359 人(1.7%)患有 cN3M0 疾病。这些患者的中位生存期为 12.5 个月(95% CI 10.7-14.3)。单纯化放疗和新辅助治疗加手术的中位生存期分别为13.3个月(95% CI 10.7-15.9)和23.7个月(95% CI 18.3-29.2)。在所有接受食管切除术的患者中,有 391 人(2.8%)患有 (y)pN3 疾病,中位 OS 为 16.1 个月(95% CI 14.8-17.4)。21名患者(5.4%)被正确分类为cN3,3年生存率为21%:结论:临床分期似乎很困难,N3食管癌患者尤其如此。手术似乎对这些患者有益。要解决临床分期和最佳新辅助治疗方面的难题,还需要更多的研究。
N3 Disease in Esophageal Cancer: Results from a Nationwide Registry.
Background: Patients with extensive lymph node metastases have a poor prognosis. Clinical staging of lymph node metastases poses significant challenges given the limited sensitivity and specificity of imaging techniques. The aim of this study was to investigate the overall survival (OS) of patients with N3 disease in a real-world Dutch population and the added value of surgery in these patients.
Methods: Patients with cN3M0 esophageal or gastroesophageal cancer were identified from the Netherlands Cancer Registry (2012-2019). Treatment consisted of neoadjuvant chemo(radio)therapy followed by resection or chemo(radio)therapy, radiotherapy, or esophagectomy alone. OS was calculated using the Kaplan-Meier method.
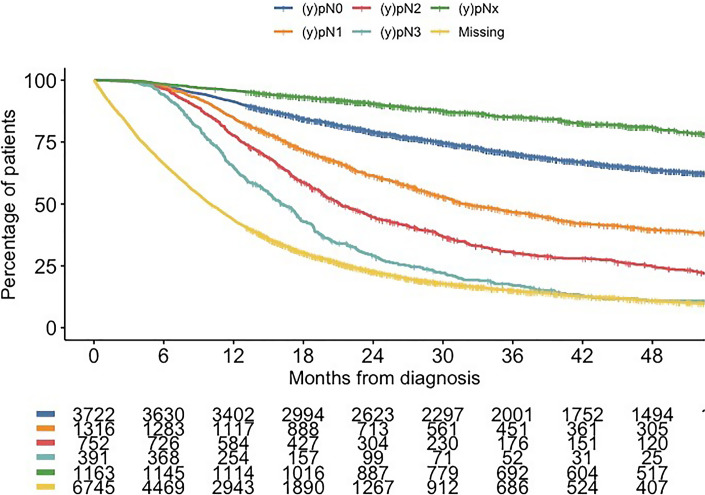
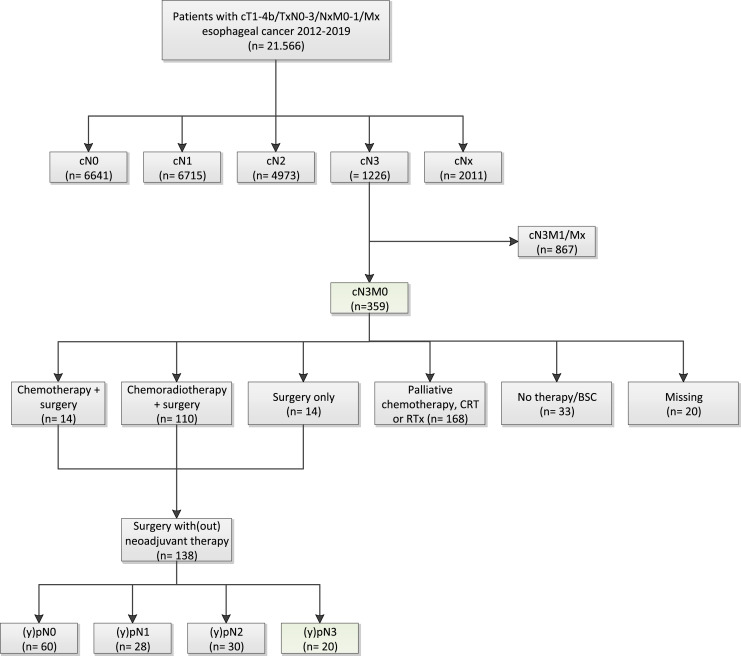
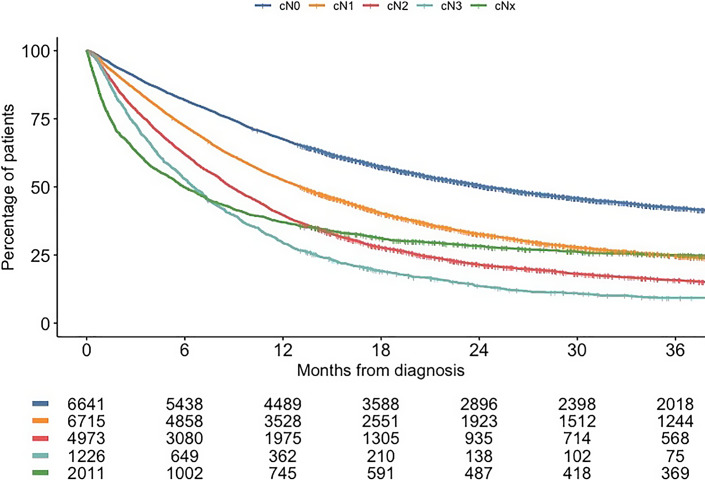
Results: Some 21,566 patients were diagnosed with esophageal cancer of whom 359 (1.7%) had cN3M0 disease. Median OS of these patients was 12.5 months (95% CI: 10.7-14.3). Median OS following chemoradiotherapy alone and neoadjuvant therapy plus surgery was 13.3 months (95% CI: 10.7-15.9) and 23.7 months (95% CI: 18.3-29.2), respectively. Of all patients who underwent esophagectomy, 391 (2.8%) had (y)pN3 disease, and median OS was 16.1 months (95% CI: 14.8-17.4). Twenty-one patients (5.4%) were correctly classified as cN3, and 3-year OS was 21%.
Conclusion(s): Clinical staging appears to be difficult, apparently in patients with N3 esophageal cancer. Surgery seems to be of benefit to these patients. More research is required to address the ongoing challenges in clinical staging and the best neoadjuvant therapy.
期刊介绍:
''Digestive Surgery'' presents a comprehensive overview in the field of gastrointestinal surgery. Interdisciplinary in scope, the journal keeps the specialist aware of advances in all fields that contribute to improvements in the diagnosis and treatment of gastrointestinal disease. Particular emphasis is given to articles that evaluate not only recent clinical developments, especially clinical trials and technical innovations such as new endoscopic and laparoscopic procedures, but also relevant translational research. Each contribution is carefully aligned with the need of the digestive surgeon. Thus, the journal is an important component of the continuing medical education of surgeons who want their practice to benefit from a familiarity with new knowledge in all its dimensions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
