José Miguel Rivera-Caravaca, Freddy Frost, Francisco Marín, Gregory Y. H. Lip
{"title":"先前口服抗凝疗法对 COVID-19 出院后疗效的影响:全球联合医疗网络分析结果。","authors":"José Miguel Rivera-Caravaca, Freddy Frost, Francisco Marín, Gregory Y. H. Lip","doi":"10.1111/eci.14299","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The impact of chronic oral anticoagulant (OACs) use on long-term post-discharge outcomes after coronavirus disease 2019 (COVID-19) hospitalisation remains unclear. Herein, we compared clinical outcomes up to 2-years after COVID-19 hospitalisation between patients on vitamin K antagonists (VKAs), direct-acting OACs (DOACs) and no OAC therapy.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Data from TriNetX, a global federated health research network, were used. Adult patients on VKAs, DOACs or no OAC therapy at diagnosis of COVID-19 between 20 January 2020 and 31 December 2021, who were hospitalised for COVID-19, were included. The primary outcomes were all-cause mortality, ischaemic stroke/transient ischaemic attack (TIA)/systemic embolism (SE) and the composite of intracranial haemorrhage (ICH)/gastrointestinal bleeding, at 2 years after COVID-19 hospitalisation.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We included 110,834 patients with COVID-19. Following propensity score matching (PSM), we identified a decreased mortality risk in DOAC-treated patients compared to the no OAC cohort (RR .808, 95% CI .751–.870). A higher risk of ischaemic stroke/TIA/SE was observed in VKA users compared to DOAC users (RR 1.100, 95% CI 1.020–1.220) and in VKA users compared to patients not taking OAC (RR 1.400, 95% CI 1.140–1.720). VKA use was associated with a greater risk of ICH/gastrointestinal bleeding than DOAC users (RR 1.198, 95% CI 1.066–1.347), while DOAC users had a lower risk compared to no OAC-treated patients (RR .840, 95% CI .754–.936).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>COVID-19 patients taking prior DOACs were associated with lower long-term mortality risk and ICH/gastrointestinal bleeding than patients not taking OAC. Compared to patients on DOACs, VKA users were associated with higher risks of mortality, ischaemic stroke/TIA/SE and ICH/gastrointestinal bleeding.</p>\n </section>\n </div>","PeriodicalId":12013,"journal":{"name":"European Journal of Clinical Investigation","volume":"54 12","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2024-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.14299","citationCount":"0","resultStr":"{\"title\":\"Impact of prior oral anticoagulation therapies on post-discharge outcomes after COVID-19: Results from a global federated health network analysis\",\"authors\":\"José Miguel Rivera-Caravaca, Freddy Frost, Francisco Marín, Gregory Y. H. Lip\",\"doi\":\"10.1111/eci.14299\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>The impact of chronic oral anticoagulant (OACs) use on long-term post-discharge outcomes after coronavirus disease 2019 (COVID-19) hospitalisation remains unclear. Herein, we compared clinical outcomes up to 2-years after COVID-19 hospitalisation between patients on vitamin K antagonists (VKAs), direct-acting OACs (DOACs) and no OAC therapy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Data from TriNetX, a global federated health research network, were used. Adult patients on VKAs, DOACs or no OAC therapy at diagnosis of COVID-19 between 20 January 2020 and 31 December 2021, who were hospitalised for COVID-19, were included. The primary outcomes were all-cause mortality, ischaemic stroke/transient ischaemic attack (TIA)/systemic embolism (SE) and the composite of intracranial haemorrhage (ICH)/gastrointestinal bleeding, at 2 years after COVID-19 hospitalisation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We included 110,834 patients with COVID-19. Following propensity score matching (PSM), we identified a decreased mortality risk in DOAC-treated patients compared to the no OAC cohort (RR .808, 95% CI .751–.870). A higher risk of ischaemic stroke/TIA/SE was observed in VKA users compared to DOAC users (RR 1.100, 95% CI 1.020–1.220) and in VKA users compared to patients not taking OAC (RR 1.400, 95% CI 1.140–1.720). VKA use was associated with a greater risk of ICH/gastrointestinal bleeding than DOAC users (RR 1.198, 95% CI 1.066–1.347), while DOAC users had a lower risk compared to no OAC-treated patients (RR .840, 95% CI .754–.936).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>COVID-19 patients taking prior DOACs were associated with lower long-term mortality risk and ICH/gastrointestinal bleeding than patients not taking OAC. Compared to patients on DOACs, VKA users were associated with higher risks of mortality, ischaemic stroke/TIA/SE and ICH/gastrointestinal bleeding.</p>\\n </section>\\n </div>\",\"PeriodicalId\":12013,\"journal\":{\"name\":\"European Journal of Clinical Investigation\",\"volume\":\"54 12\",\"pages\":\"\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2024-08-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.14299\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Clinical Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/eci.14299\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/eci.14299","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Impact of prior oral anticoagulation therapies on post-discharge outcomes after COVID-19: Results from a global federated health network analysis
Background
The impact of chronic oral anticoagulant (OACs) use on long-term post-discharge outcomes after coronavirus disease 2019 (COVID-19) hospitalisation remains unclear. Herein, we compared clinical outcomes up to 2-years after COVID-19 hospitalisation between patients on vitamin K antagonists (VKAs), direct-acting OACs (DOACs) and no OAC therapy.
Methods
Data from TriNetX, a global federated health research network, were used. Adult patients on VKAs, DOACs or no OAC therapy at diagnosis of COVID-19 between 20 January 2020 and 31 December 2021, who were hospitalised for COVID-19, were included. The primary outcomes were all-cause mortality, ischaemic stroke/transient ischaemic attack (TIA)/systemic embolism (SE) and the composite of intracranial haemorrhage (ICH)/gastrointestinal bleeding, at 2 years after COVID-19 hospitalisation.
Results
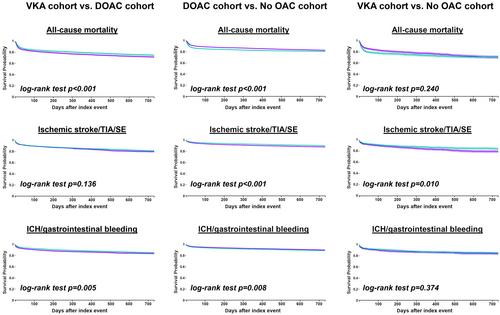
We included 110,834 patients with COVID-19. Following propensity score matching (PSM), we identified a decreased mortality risk in DOAC-treated patients compared to the no OAC cohort (RR .808, 95% CI .751–.870). A higher risk of ischaemic stroke/TIA/SE was observed in VKA users compared to DOAC users (RR 1.100, 95% CI 1.020–1.220) and in VKA users compared to patients not taking OAC (RR 1.400, 95% CI 1.140–1.720). VKA use was associated with a greater risk of ICH/gastrointestinal bleeding than DOAC users (RR 1.198, 95% CI 1.066–1.347), while DOAC users had a lower risk compared to no OAC-treated patients (RR .840, 95% CI .754–.936).
Conclusion
COVID-19 patients taking prior DOACs were associated with lower long-term mortality risk and ICH/gastrointestinal bleeding than patients not taking OAC. Compared to patients on DOACs, VKA users were associated with higher risks of mortality, ischaemic stroke/TIA/SE and ICH/gastrointestinal bleeding.
期刊介绍:
EJCI considers any original contribution from the most sophisticated basic molecular sciences to applied clinical and translational research and evidence-based medicine across a broad range of subspecialties. The EJCI publishes reports of high-quality research that pertain to the genetic, molecular, cellular, or physiological basis of human biology and disease, as well as research that addresses prevalence, diagnosis, course, treatment, and prevention of disease. We are primarily interested in studies directly pertinent to humans, but submission of robust in vitro and animal work is also encouraged. Interdisciplinary work and research using innovative methods and combinations of laboratory, clinical, and epidemiological methodologies and techniques is of great interest to the journal. Several categories of manuscripts (for detailed description see below) are considered: editorials, original articles (also including randomized clinical trials, systematic reviews and meta-analyses), reviews (narrative reviews), opinion articles (including debates, perspectives and commentaries); and letters to the Editor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
