Mitchell T. Victor BA, Farhoud Faraji MD, PhD, Rohith Voora MD, Sandhya Kalavacherla BS, Loren K. Mell MD, Brent S. Rose MD, Theresa W. Guo MD
{"title":"喉癌保留器官治疗后进行全喉切除术的相关因素。","authors":"Mitchell T. Victor BA, Farhoud Faraji MD, PhD, Rohith Voora MD, Sandhya Kalavacherla BS, Loren K. Mell MD, Brent S. Rose MD, Theresa W. Guo MD","doi":"10.1002/lio2.1317","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective(s)</h3>\n \n <p>A subset of laryngeal squamous cell carcinoma (LSCC) patients undergoing larynx preserving treatment ultimately require total laryngectomy (TL) for oncologic or functional reasons. This study aims to identify TL risk factors in these patients.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Retrospective cohort study using Veterans Affairs (VA) database. T1–T4 LSCC cases treated with primary radiotherapy (XRT) or chemoradiotherapy (CRT) were assessed for TL and recurrence. Binary logistic and Cox regression and Kaplan–Meier analyses were implemented.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 5390 cases, 863 (16.0%) underwent TL. On multivariable analysis, age (adjusted odds ratio: 0.97 [0.96–0.98]; <i>p</i> < .001) and N3 disease (0.42 [0.18–1.00]; <i>p</i> = .050) were associated with reduced risk of TL, whereas current alcohol use (1.22 [1.04–1.43]; <i>p</i> = .015) and >T1 disease (T2, 1.76 [1.44–2.17]; <i>p</i> < .001; T3, 2.06 [1.58–2.68]; <i>p</i> < .001; T4, 1.79 [1.26–2.53]; <i>p</i> = .001) were associated with increased risk of TL. However, N2 (adjusted hazard ratio: 1.30 [1.10–1.55]; <i>p</i> = .003) and N3 (2.02 [1.25–3.26]; <i>p</i> = .004) disease were associated with an increased risk for local recurrence. Compared to XRT, treatment with CRT was associated with reduced risk for local recurrence after adjusting for other factors (0.84 [0.70–0.99]; <i>p</i> = .044). Those who do not receive TL following local recurrence have poorer disease-specific survival (log-rank, <i>p</i> < .001). In patients without local recurrence, N2 disease was associated with a fourfold increase in risk of TL (4.24 [1.83–9.82]; <i>p</i> < .001).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Advanced nodal stage was associated with reduced rates of salvage TL in the setting of local recurrence, and subsequent worse prognosis after recurrence. Conversely, advanced nodal stage may increase the risk for functional salvage TL in patients without recurrence.</p>\n </section>\n \n <section>\n \n <h3> Level of Evidence</h3>\n \n <p>Level 3.</p>\n </section>\n </div>","PeriodicalId":48529,"journal":{"name":"Laryngoscope Investigative Otolaryngology","volume":"9 4","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2024-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11301822/pdf/","citationCount":"0","resultStr":"{\"title\":\"Factors associated with total laryngectomy following organ-preserving treatment of laryngeal SCC\",\"authors\":\"Mitchell T. Victor BA, Farhoud Faraji MD, PhD, Rohith Voora MD, Sandhya Kalavacherla BS, Loren K. Mell MD, Brent S. Rose MD, Theresa W. Guo MD\",\"doi\":\"10.1002/lio2.1317\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective(s)</h3>\\n \\n <p>A subset of laryngeal squamous cell carcinoma (LSCC) patients undergoing larynx preserving treatment ultimately require total laryngectomy (TL) for oncologic or functional reasons. This study aims to identify TL risk factors in these patients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Retrospective cohort study using Veterans Affairs (VA) database. T1–T4 LSCC cases treated with primary radiotherapy (XRT) or chemoradiotherapy (CRT) were assessed for TL and recurrence. Binary logistic and Cox regression and Kaplan–Meier analyses were implemented.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 5390 cases, 863 (16.0%) underwent TL. On multivariable analysis, age (adjusted odds ratio: 0.97 [0.96–0.98]; <i>p</i> < .001) and N3 disease (0.42 [0.18–1.00]; <i>p</i> = .050) were associated with reduced risk of TL, whereas current alcohol use (1.22 [1.04–1.43]; <i>p</i> = .015) and >T1 disease (T2, 1.76 [1.44–2.17]; <i>p</i> < .001; T3, 2.06 [1.58–2.68]; <i>p</i> < .001; T4, 1.79 [1.26–2.53]; <i>p</i> = .001) were associated with increased risk of TL. However, N2 (adjusted hazard ratio: 1.30 [1.10–1.55]; <i>p</i> = .003) and N3 (2.02 [1.25–3.26]; <i>p</i> = .004) disease were associated with an increased risk for local recurrence. Compared to XRT, treatment with CRT was associated with reduced risk for local recurrence after adjusting for other factors (0.84 [0.70–0.99]; <i>p</i> = .044). Those who do not receive TL following local recurrence have poorer disease-specific survival (log-rank, <i>p</i> < .001). In patients without local recurrence, N2 disease was associated with a fourfold increase in risk of TL (4.24 [1.83–9.82]; <i>p</i> < .001).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Advanced nodal stage was associated with reduced rates of salvage TL in the setting of local recurrence, and subsequent worse prognosis after recurrence. Conversely, advanced nodal stage may increase the risk for functional salvage TL in patients without recurrence.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Level of Evidence</h3>\\n \\n <p>Level 3.</p>\\n </section>\\n </div>\",\"PeriodicalId\":48529,\"journal\":{\"name\":\"Laryngoscope Investigative Otolaryngology\",\"volume\":\"9 4\",\"pages\":\"\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-08-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11301822/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Laryngoscope Investigative Otolaryngology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lio2.1317\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Laryngoscope Investigative Otolaryngology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lio2.1317","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:在接受保喉治疗的喉鳞状细胞癌(LSCC)患者中,有一部分患者最终因肿瘤或功能原因需要进行全喉切除术(TL)。本研究旨在确定这些患者的全喉切除风险因素:使用退伍军人事务(VA)数据库进行回顾性队列研究。对接受原发性放疗(XRT)或化放疗(CRT)治疗的T1-T4 LSCC病例进行TL和复发评估。采用二元逻辑回归、Cox回归和Kaplan-Meier分析:在 5390 例病例中,863 例(16.0%)接受了 TL 治疗。在多变量分析中,年龄(调整后的几率比:0.97 [0.96-0.98];p p = .050)与 TL 风险降低有关,而当前饮酒(1.22 [1.04-1.43];p = .015)和 >T1 疾病(T2,1.76 [1.44-2.17];p p p = .001)与 TL 风险增加有关。然而,N2(调整后危险比:1.30 [1.10-1.55];p = .003)和 N3(2.02 [1.25-3.26];p = .004)疾病与局部复发风险增加有关。与 XRT 相比,在调整其他因素后,CRT 治疗与局部复发风险降低相关(0.84 [0.70-0.99]; p = .044)。局部复发后未接受 TL 治疗者的疾病特异性生存率较低(对数秩,p p 结论):晚期结节分期与局部复发时TL挽救率降低以及复发后预后较差有关。相反,晚期结节分期可能会增加无复发患者功能性挽救性 TL 的风险:证据等级:3级。
Factors associated with total laryngectomy following organ-preserving treatment of laryngeal SCC
Objective(s)
A subset of laryngeal squamous cell carcinoma (LSCC) patients undergoing larynx preserving treatment ultimately require total laryngectomy (TL) for oncologic or functional reasons. This study aims to identify TL risk factors in these patients.
Methods
Retrospective cohort study using Veterans Affairs (VA) database. T1–T4 LSCC cases treated with primary radiotherapy (XRT) or chemoradiotherapy (CRT) were assessed for TL and recurrence. Binary logistic and Cox regression and Kaplan–Meier analyses were implemented.
Results
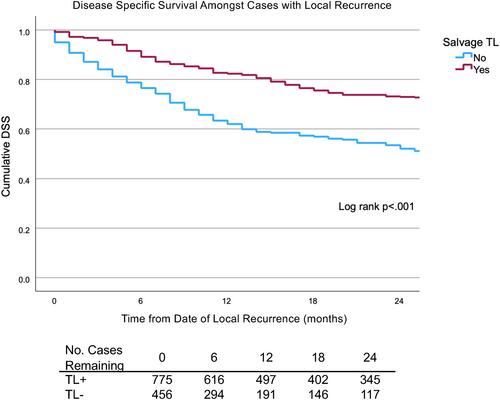
Of 5390 cases, 863 (16.0%) underwent TL. On multivariable analysis, age (adjusted odds ratio: 0.97 [0.96–0.98]; p < .001) and N3 disease (0.42 [0.18–1.00]; p = .050) were associated with reduced risk of TL, whereas current alcohol use (1.22 [1.04–1.43]; p = .015) and >T1 disease (T2, 1.76 [1.44–2.17]; p < .001; T3, 2.06 [1.58–2.68]; p < .001; T4, 1.79 [1.26–2.53]; p = .001) were associated with increased risk of TL. However, N2 (adjusted hazard ratio: 1.30 [1.10–1.55]; p = .003) and N3 (2.02 [1.25–3.26]; p = .004) disease were associated with an increased risk for local recurrence. Compared to XRT, treatment with CRT was associated with reduced risk for local recurrence after adjusting for other factors (0.84 [0.70–0.99]; p = .044). Those who do not receive TL following local recurrence have poorer disease-specific survival (log-rank, p < .001). In patients without local recurrence, N2 disease was associated with a fourfold increase in risk of TL (4.24 [1.83–9.82]; p < .001).
Conclusion
Advanced nodal stage was associated with reduced rates of salvage TL in the setting of local recurrence, and subsequent worse prognosis after recurrence. Conversely, advanced nodal stage may increase the risk for functional salvage TL in patients without recurrence.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
