Lucy Plumb, Retha Steenkamp, Alexander J Hamilton, Heather Maxwell, Carol D Inward, Stephen D Marks, Dorothea Nitsch
{"title":"利用登记和链接的电子健康记录数据分析已确诊肾衰竭儿童的并存疾病谱。","authors":"Lucy Plumb, Retha Steenkamp, Alexander J Hamilton, Heather Maxwell, Carol D Inward, Stephen D Marks, Dorothea Nitsch","doi":"10.1007/s00467-024-06470-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Children with established kidney failure may have additional medical conditions influencing kidney care and outcomes. This cross-sectional study aimed to examine the prevalence of co-existing diseases captured in the electronic hospital record compared to UK Renal Registry (UKRR) data and differences in coding.</p><p><strong>Methods: </strong>The study population comprised children aged < 18 years receiving kidney replacement therapy (KRT) in England and Wales on 31/12/2016. Comorbidity data at KRT start was examined in the hospital record and compared to UKRR data. Agreement was assessed by the kappa statistic. Associations between patient and clinical factors and likelihood of coding were examined using multivariable logistic regression.</p><p><strong>Results: </strong>A total of 869 children (62.5% male) had data linkage for inclusion. UKRR records generally reported a higher prevalence of co-existing disease than electronic health records; congenital, non-kidney disease was most commonly reported across both datasets. The highest sensitivity in the hospital record was seen for congenital heart disease (odds ratio (OR) 0.65, 95% confidence interval (CI) 0.51, 0.78) and malignancy (OR 0.63, 95% CI 0.41, 0.85). At best, moderate agreement (kappa ≥ 0.41) was seen between the datasets. Factors associated with higher odds of coding in hospital records included age, while kidney disease and a higher number of comorbidities were associated with lower odds of coding.</p><p><strong>Conclusions: </strong>Health records generally under-reported co-existing disease compared to registry data with fair-moderate agreement between datasets. Electronic health records offer a non-selective overview of co-existing disease facilitating audit and research, but registry processes are still required to capture paediatric-specific variables pertinent to kidney disease.</p>","PeriodicalId":19735,"journal":{"name":"Pediatric Nephrology","volume":" ","pages":"3521-3531"},"PeriodicalIF":2.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11511698/pdf/","citationCount":"0","resultStr":"{\"title\":\"The spectrum of co-existing disease in children with established kidney failure using registry and linked electronic health record data.\",\"authors\":\"Lucy Plumb, Retha Steenkamp, Alexander J Hamilton, Heather Maxwell, Carol D Inward, Stephen D Marks, Dorothea Nitsch\",\"doi\":\"10.1007/s00467-024-06470-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Children with established kidney failure may have additional medical conditions influencing kidney care and outcomes. This cross-sectional study aimed to examine the prevalence of co-existing diseases captured in the electronic hospital record compared to UK Renal Registry (UKRR) data and differences in coding.</p><p><strong>Methods: </strong>The study population comprised children aged < 18 years receiving kidney replacement therapy (KRT) in England and Wales on 31/12/2016. Comorbidity data at KRT start was examined in the hospital record and compared to UKRR data. Agreement was assessed by the kappa statistic. Associations between patient and clinical factors and likelihood of coding were examined using multivariable logistic regression.</p><p><strong>Results: </strong>A total of 869 children (62.5% male) had data linkage for inclusion. UKRR records generally reported a higher prevalence of co-existing disease than electronic health records; congenital, non-kidney disease was most commonly reported across both datasets. The highest sensitivity in the hospital record was seen for congenital heart disease (odds ratio (OR) 0.65, 95% confidence interval (CI) 0.51, 0.78) and malignancy (OR 0.63, 95% CI 0.41, 0.85). At best, moderate agreement (kappa ≥ 0.41) was seen between the datasets. Factors associated with higher odds of coding in hospital records included age, while kidney disease and a higher number of comorbidities were associated with lower odds of coding.</p><p><strong>Conclusions: </strong>Health records generally under-reported co-existing disease compared to registry data with fair-moderate agreement between datasets. Electronic health records offer a non-selective overview of co-existing disease facilitating audit and research, but registry processes are still required to capture paediatric-specific variables pertinent to kidney disease.</p>\",\"PeriodicalId\":19735,\"journal\":{\"name\":\"Pediatric Nephrology\",\"volume\":\" \",\"pages\":\"3521-3531\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11511698/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Nephrology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00467-024-06470-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00467-024-06470-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/8 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
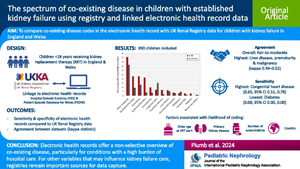
The spectrum of co-existing disease in children with established kidney failure using registry and linked electronic health record data.
Background: Children with established kidney failure may have additional medical conditions influencing kidney care and outcomes. This cross-sectional study aimed to examine the prevalence of co-existing diseases captured in the electronic hospital record compared to UK Renal Registry (UKRR) data and differences in coding.
Methods: The study population comprised children aged < 18 years receiving kidney replacement therapy (KRT) in England and Wales on 31/12/2016. Comorbidity data at KRT start was examined in the hospital record and compared to UKRR data. Agreement was assessed by the kappa statistic. Associations between patient and clinical factors and likelihood of coding were examined using multivariable logistic regression.
Results: A total of 869 children (62.5% male) had data linkage for inclusion. UKRR records generally reported a higher prevalence of co-existing disease than electronic health records; congenital, non-kidney disease was most commonly reported across both datasets. The highest sensitivity in the hospital record was seen for congenital heart disease (odds ratio (OR) 0.65, 95% confidence interval (CI) 0.51, 0.78) and malignancy (OR 0.63, 95% CI 0.41, 0.85). At best, moderate agreement (kappa ≥ 0.41) was seen between the datasets. Factors associated with higher odds of coding in hospital records included age, while kidney disease and a higher number of comorbidities were associated with lower odds of coding.
Conclusions: Health records generally under-reported co-existing disease compared to registry data with fair-moderate agreement between datasets. Electronic health records offer a non-selective overview of co-existing disease facilitating audit and research, but registry processes are still required to capture paediatric-specific variables pertinent to kidney disease.
期刊介绍:
International Pediatric Nephrology Association
Pediatric Nephrology publishes original clinical research related to acute and chronic diseases that affect renal function, blood pressure, and fluid and electrolyte disorders in children. Studies may involve medical, surgical, nutritional, physiologic, biochemical, genetic, pathologic or immunologic aspects of disease, imaging techniques or consequences of acute or chronic kidney disease. There are 12 issues per year that contain Editorial Commentaries, Reviews, Educational Reviews, Original Articles, Brief Reports, Rapid Communications, Clinical Quizzes, and Letters to the Editors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
