Simone Arnold, Manuela Nickler, Michael Dickenmann, Thomas Menter, Helmut Hopfer, Patricia Hirt-Minkowski
{"title":"伊帕克潘首次成功治疗原发性免疫复合物-膜增生性肾小球肾炎患者:病例报告。","authors":"Simone Arnold, Manuela Nickler, Michael Dickenmann, Thomas Menter, Helmut Hopfer, Patricia Hirt-Minkowski","doi":"10.1159/000540013","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Nowadays, there is insufficient evidence for the recommendation of management patients with a primary membranoproliferative glomerulonephritis (MPGN). A better understanding of the pathogenesis has led to the reclassification of primary MPGN and distinction into the two main entities of either primary immune complex-MPGN or C3 glomerulopathy. Both entities share overlapping pathophysiological features with complement alternative pathway (AP) dysregulation. Iptacopan is an oral inhibitor of the complement factor B that effectively blocks the complement AP.</p><p><strong>Case presentation: </strong>We report the first successful treatment of a 47-year-old man suffering from a primary immune complex-MPGN with iptacopan. So far established immunosuppressive therapies with prednisone and mycophenolate mofetil failed to control the current flare of the disease, mainly presenting with impaired kidney function and proteinuria within the nephrotic range. However, 3 months after starting the treatment with iptacopan urine protein-creatinine ratio decreased impressively to a level of 100-150 mg/mmol. Thereafter, low-level proteinuria and kidney function remained stable during follow-up. Do date, the treatment with iptacopan is continued as a monotherapy and is well tolerated.</p><p><strong>Conclusion: </strong>To the best of our knowledge, this is the first case report which suggests that iptacopan may be an interesting treatment option for primary immune complex-MPGN.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"14 1","pages":"138-147"},"PeriodicalIF":1.0000,"publicationDate":"2024-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11309753/pdf/","citationCount":"0","resultStr":"{\"title\":\"First Successful Treatment of a Patient with a Primary Immune Complex-Membranoproliferative Glomerulonephritis with Iptacopan: A Case Report.\",\"authors\":\"Simone Arnold, Manuela Nickler, Michael Dickenmann, Thomas Menter, Helmut Hopfer, Patricia Hirt-Minkowski\",\"doi\":\"10.1159/000540013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Nowadays, there is insufficient evidence for the recommendation of management patients with a primary membranoproliferative glomerulonephritis (MPGN). A better understanding of the pathogenesis has led to the reclassification of primary MPGN and distinction into the two main entities of either primary immune complex-MPGN or C3 glomerulopathy. Both entities share overlapping pathophysiological features with complement alternative pathway (AP) dysregulation. Iptacopan is an oral inhibitor of the complement factor B that effectively blocks the complement AP.</p><p><strong>Case presentation: </strong>We report the first successful treatment of a 47-year-old man suffering from a primary immune complex-MPGN with iptacopan. So far established immunosuppressive therapies with prednisone and mycophenolate mofetil failed to control the current flare of the disease, mainly presenting with impaired kidney function and proteinuria within the nephrotic range. However, 3 months after starting the treatment with iptacopan urine protein-creatinine ratio decreased impressively to a level of 100-150 mg/mmol. Thereafter, low-level proteinuria and kidney function remained stable during follow-up. Do date, the treatment with iptacopan is continued as a monotherapy and is well tolerated.</p><p><strong>Conclusion: </strong>To the best of our knowledge, this is the first case report which suggests that iptacopan may be an interesting treatment option for primary immune complex-MPGN.</p>\",\"PeriodicalId\":9599,\"journal\":{\"name\":\"Case Reports in Nephrology and Dialysis\",\"volume\":\"14 1\",\"pages\":\"138-147\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11309753/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Nephrology and Dialysis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000540013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000540013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
First Successful Treatment of a Patient with a Primary Immune Complex-Membranoproliferative Glomerulonephritis with Iptacopan: A Case Report.
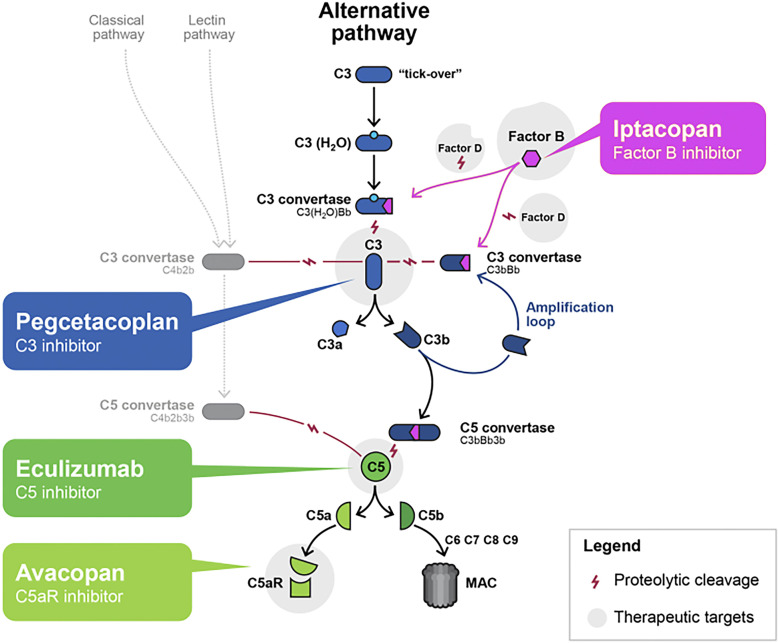
Introduction: Nowadays, there is insufficient evidence for the recommendation of management patients with a primary membranoproliferative glomerulonephritis (MPGN). A better understanding of the pathogenesis has led to the reclassification of primary MPGN and distinction into the two main entities of either primary immune complex-MPGN or C3 glomerulopathy. Both entities share overlapping pathophysiological features with complement alternative pathway (AP) dysregulation. Iptacopan is an oral inhibitor of the complement factor B that effectively blocks the complement AP.
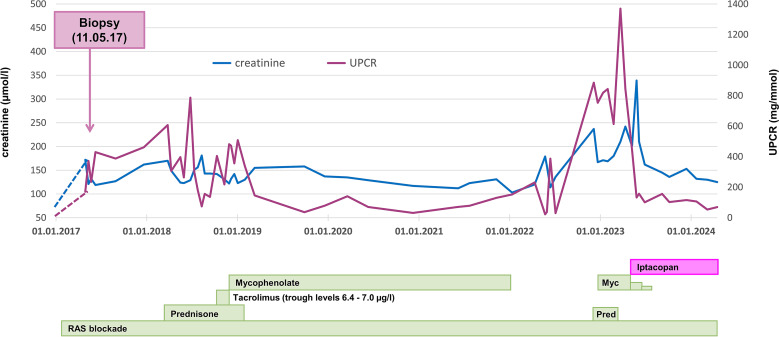
Case presentation: We report the first successful treatment of a 47-year-old man suffering from a primary immune complex-MPGN with iptacopan. So far established immunosuppressive therapies with prednisone and mycophenolate mofetil failed to control the current flare of the disease, mainly presenting with impaired kidney function and proteinuria within the nephrotic range. However, 3 months after starting the treatment with iptacopan urine protein-creatinine ratio decreased impressively to a level of 100-150 mg/mmol. Thereafter, low-level proteinuria and kidney function remained stable during follow-up. Do date, the treatment with iptacopan is continued as a monotherapy and is well tolerated.
Conclusion: To the best of our knowledge, this is the first case report which suggests that iptacopan may be an interesting treatment option for primary immune complex-MPGN.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
