Mahender Yadagiri, Fiona Y. Kinney, Natalie Ashman, John P. Bleasdale, Edward N. Fogden, Mark R. Anderson, Christopher Walton, Michael A. Greenstone, Robert E. J. Ryder
{"title":"内镜十二指肠空肠分流术治疗中度阻塞性睡眠呼吸暂停--一项试验研究。","authors":"Mahender Yadagiri, Fiona Y. Kinney, Natalie Ashman, John P. Bleasdale, Edward N. Fogden, Mark R. Anderson, Christopher Walton, Michael A. Greenstone, Robert E. J. Ryder","doi":"10.1111/cob.12694","DOIUrl":null,"url":null,"abstract":"<p>We aimed to assess the extent to which people with type 2 diabetes or pre-diabetes, obesity (BMI 30–45 kg/m<sup>2</sup>) and moderate obstructive sleep apnoea (OSA) requiring continuous positive airway pressure ventilation (CPAP) were able to discontinue CPAP following EndoBarrier-related weight loss. We assessed sleep and metabolic parameters before, during and after EndoBarrier in 12 participants with moderate OSA requiring CPAP (75% female, 8/12 [66%] type 2 diabetes, 4/12 [34%] prediabetes, mean ± SD age 52.6 ± 9.7 years, BMI 37.4 ± 3.5 kg/m<sup>2</sup>, median duration of OSA while on CPAP 9.0 [7.0–15.0] months). With EndoBarrier in-situ, mean ± SD Apnoea Hypopnoea Index (AHI) fell by 9.1 ± 5.0 events/h from 18.9 ± 3.8 to 9.7 ± 3.0 events/h (<i>p</i> < .001) with an associated reduction in symptoms of daytime sleepiness (mean Epworth Sleepiness Score) such that all the 12 participants no longer required CPAP according to National Institute for Health and Care Excellence criteria. After EndoBarrier removal, 10/12 (83%) patients attended follow-up and at 12 months after removal, AHI remained below 15 in 5/10 (50%) patients but in other five the AHI rose above 15 such that restarting CPAP was recommended as justified by their symptoms. Rather than restart CPAP, two patients lost the regained weight and their AHI dropped below 15 again. Thus, 7/10 (70%) of patients were able to remain off CPAP 12 or more months after EndoBarrier removal. These results demonstrate major benefit of EndoBarrier in moderate OSA, allowing all patients to discontinue CPAP during treatment, and with maintenance of improvement at follow-up in 70%. They confirm previously demonstrated metabolic improvements in diabetes and obesity.</p>","PeriodicalId":10399,"journal":{"name":"Clinical Obesity","volume":"14 6","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2024-08-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cob.12694","citationCount":"0","resultStr":"{\"title\":\"Endoscopic duodenal-jejunal bypass liner treatment of moderate obstructive sleep apnoea—A pilot study\",\"authors\":\"Mahender Yadagiri, Fiona Y. Kinney, Natalie Ashman, John P. Bleasdale, Edward N. Fogden, Mark R. Anderson, Christopher Walton, Michael A. Greenstone, Robert E. J. Ryder\",\"doi\":\"10.1111/cob.12694\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>We aimed to assess the extent to which people with type 2 diabetes or pre-diabetes, obesity (BMI 30–45 kg/m<sup>2</sup>) and moderate obstructive sleep apnoea (OSA) requiring continuous positive airway pressure ventilation (CPAP) were able to discontinue CPAP following EndoBarrier-related weight loss. We assessed sleep and metabolic parameters before, during and after EndoBarrier in 12 participants with moderate OSA requiring CPAP (75% female, 8/12 [66%] type 2 diabetes, 4/12 [34%] prediabetes, mean ± SD age 52.6 ± 9.7 years, BMI 37.4 ± 3.5 kg/m<sup>2</sup>, median duration of OSA while on CPAP 9.0 [7.0–15.0] months). With EndoBarrier in-situ, mean ± SD Apnoea Hypopnoea Index (AHI) fell by 9.1 ± 5.0 events/h from 18.9 ± 3.8 to 9.7 ± 3.0 events/h (<i>p</i> < .001) with an associated reduction in symptoms of daytime sleepiness (mean Epworth Sleepiness Score) such that all the 12 participants no longer required CPAP according to National Institute for Health and Care Excellence criteria. After EndoBarrier removal, 10/12 (83%) patients attended follow-up and at 12 months after removal, AHI remained below 15 in 5/10 (50%) patients but in other five the AHI rose above 15 such that restarting CPAP was recommended as justified by their symptoms. Rather than restart CPAP, two patients lost the regained weight and their AHI dropped below 15 again. Thus, 7/10 (70%) of patients were able to remain off CPAP 12 or more months after EndoBarrier removal. These results demonstrate major benefit of EndoBarrier in moderate OSA, allowing all patients to discontinue CPAP during treatment, and with maintenance of improvement at follow-up in 70%. They confirm previously demonstrated metabolic improvements in diabetes and obesity.</p>\",\"PeriodicalId\":10399,\"journal\":{\"name\":\"Clinical Obesity\",\"volume\":\"14 6\",\"pages\":\"\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-08-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cob.12694\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Obesity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cob.12694\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Obesity","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cob.12694","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Endoscopic duodenal-jejunal bypass liner treatment of moderate obstructive sleep apnoea—A pilot study
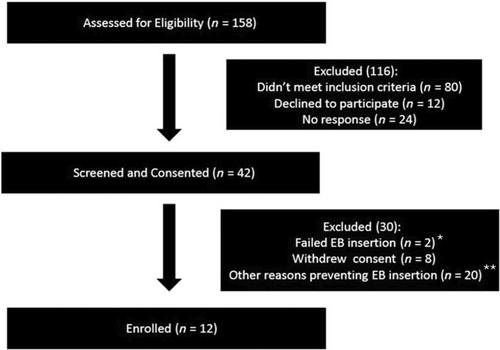
We aimed to assess the extent to which people with type 2 diabetes or pre-diabetes, obesity (BMI 30–45 kg/m2) and moderate obstructive sleep apnoea (OSA) requiring continuous positive airway pressure ventilation (CPAP) were able to discontinue CPAP following EndoBarrier-related weight loss. We assessed sleep and metabolic parameters before, during and after EndoBarrier in 12 participants with moderate OSA requiring CPAP (75% female, 8/12 [66%] type 2 diabetes, 4/12 [34%] prediabetes, mean ± SD age 52.6 ± 9.7 years, BMI 37.4 ± 3.5 kg/m2, median duration of OSA while on CPAP 9.0 [7.0–15.0] months). With EndoBarrier in-situ, mean ± SD Apnoea Hypopnoea Index (AHI) fell by 9.1 ± 5.0 events/h from 18.9 ± 3.8 to 9.7 ± 3.0 events/h (p < .001) with an associated reduction in symptoms of daytime sleepiness (mean Epworth Sleepiness Score) such that all the 12 participants no longer required CPAP according to National Institute for Health and Care Excellence criteria. After EndoBarrier removal, 10/12 (83%) patients attended follow-up and at 12 months after removal, AHI remained below 15 in 5/10 (50%) patients but in other five the AHI rose above 15 such that restarting CPAP was recommended as justified by their symptoms. Rather than restart CPAP, two patients lost the regained weight and their AHI dropped below 15 again. Thus, 7/10 (70%) of patients were able to remain off CPAP 12 or more months after EndoBarrier removal. These results demonstrate major benefit of EndoBarrier in moderate OSA, allowing all patients to discontinue CPAP during treatment, and with maintenance of improvement at follow-up in 70%. They confirm previously demonstrated metabolic improvements in diabetes and obesity.
期刊介绍:
Clinical Obesity is an international peer-reviewed journal publishing high quality translational and clinical research papers and reviews focussing on obesity and its co-morbidities. Key areas of interest are: • Patient assessment, classification, diagnosis and prognosis • Drug treatments, clinical trials and supporting research • Bariatric surgery and follow-up issues • Surgical approaches to remove body fat • Pharmacological, dietary and behavioural approaches for weight loss • Clinical physiology • Clinically relevant epidemiology • Psychological aspects of obesity • Co-morbidities • Nursing and care of patients with obesity.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
