Emma J. Sailor-Longsworth, Richard D. Lutze, Matthew A. Ingersoll, Regina G. Kelmann, Kristina Ly, Duane Currier, Taosheng Chen, Jian Zuo, Tal Teitz
{"title":"常用的抗病毒药物奥司他韦(特敏福)可减轻小鼠的听力损失。","authors":"Emma J. Sailor-Longsworth, Richard D. Lutze, Matthew A. Ingersoll, Regina G. Kelmann, Kristina Ly, Duane Currier, Taosheng Chen, Jian Zuo, Tal Teitz","doi":"10.1002/ctm2.1803","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Hearing loss affects up to 10% of people worldwide and therapeutic interventions are desperately needed. Noise exposure and chemotherapy treatments are leading causes of this impairment, but currently there is only one FDA-approved drug for a subgroup of cisplatin-treated cancer patients.<span><sup>1, 2</sup></span> Hearing loss can arise from damage to many different inner ear cell types with outer hair cell (OHC) and synaptic dysfunction as two of the most common aetiologies of hearing loss.<span><sup>2-4</sup></span> Drug repurposing is a strategy for addressing unmet medical needs that can be quicker and more cost-effective than traditional drug development.<span><sup>3</sup></span> Here, we performed unbiased cell-based screens of 1300 FDA-approved drugs and tested our top candidate oseltamivir phosphate (brand name Tamiflu), a common influenza antiviral drug, in established cisplatin- and noise-induced hearing loss animal models. Our results support oseltamivir as a promising otoprotective therapeutic candidate for both cisplatin chemotherapy and traumatic noise exposure.</p><p>Oseltamivir phosphate and its active form, oseltamivir carboxylate, protect against cisplatin-induced hair cell loss in mouse cochlear explants without interfering with cisplatin's tumour killing efficacy in tumour cell lines. The prodrug, oseltamivir phosphate, tested at a dose of 3 µM, was a top hit in high-throughput screens reducing 95% of the caspase-3/7 cell death activity of cisplatin-treated cells.<span><sup>3, 4</sup></span> In mouse P3 cochlear explants, the prodrug, oseltamivir phosphate, protected from cisplatin-induced OHC death with an EC<sub>50</sub> of 450 nM (Figure 1A,D), while the active antiviral drug, oseltamivir carboxylate (Figure 1B), had a similar EC<sub>50</sub> of 505 nM (Figure 1C,E). Importantly, oseltamivir cotreatment in three small cell lung carcinoma and three neuroblastoma cell lines did not interfere with cisplatin's ability to kill tumour cells (Figure 1F–K).</p><p>Oseltamivir protects mice from cisplatin ototoxicity after a single, high dose of cisplatin and in a clinically relevant, multicycle cisplatin protocol. Adult FVB/NJ mice were treated orally with 50 mg/kg oseltamivir phosphate, 45 min before one dose of 30 mg/kg cisplatin (Figure 2A). We measured auditory brainstem response (ABR) as a test of hearing function. ABR measures nerve electrical activities from the cochleae to the brain. The ABR threshold is the lowest decibel sound pressure level (dB SPL) an animal can hear at. Mice cotreated with oseltamivir and cisplatin had 15 dB lower ABR threshold shifts at the 32 kHz region and displayed reduction in OHC death at the middle and basal cochlear regions compared to cisplatin-treated mice (Figure 2B–E). Utilising a clinically relevant multicycle cisplatin mouse model that mimics cisplatin treatment in humans (Figure 2F),<span><sup>4-6</sup></span> mice were treated orally with 50, 10 or 2 mg/kg oseltamivir, 45 min before the cisplatin treatment in the morning and 12 h later for three consecutive days. An amount of 3 mg/kg of cisplatin was administered via intraperitoneal injection. Mice cotreated with 50 and 10 mg/kg oseltamivir had significantly lower ABR threshold shifts at the 16 and 32 kHz regions, while 2 mg/kg oseltamivir treatment had no difference compared to cisplatin alone (Figure 2G,H). The 50 and 10 mg/kg oseltamivir cotreated mice with cisplatin had significantly higher ABR wave 1 amplitudes at 90 dB (Figure 2L), but no reduction in distortion product otoacoustic emission (DPOAE) threshold shifts (Figure 2I). The 50 and 10 mg/kg oseltamivir cotreatments conferred a significant reduction in OHCs loss (Figure 2J,K) and no significant difference in weight loss compared to cisplatin alone (Figure 2M).</p><p>Oral oseltamivir therapy protects against noise-induced ABR threshold shifts and cochlear synaptopathy. Mice, females or males, who received 100 mg/kg oseltamivir phosphate 24 h after noise exposure (Figure 3A) exhibited significantly reduced ABR threshold shifts relative to carrier-treated mice (Figure 3B–D). Mice that received 50 mg/kg oseltamivir had significant protection at 8 kHz (Figure 3E). No ABR protection was observed in the 10 mg/kg oseltamivir treatment group (Figure 3F). No treatment group exhibited protection from DPOAE threshold shifts (Figure 3G–I). Three-day oseltamivir treatment was sufficient for maximum otoprotective effects when initiated up to 24 h after 100 dB, 2-h noise exposure, but no protection was achieved with 106 dB, 2-h noise insult (Figure S1).</p><p>Mice treated with 100 mg/kg oseltamivir portrayed significantly higher average ABR wave 1 amplitude at 90 and 80 dB SPL and higher number of Ctbp2 inner hair cell synaptic puncta relative to carrier-treated noise exposed mice (Figure 3J–L).</p><p>Oseltamivir cisplatin otoprotection is partially mediated through inhibition of pERK protein levels and is associated with reduction in CD45-positive immune cells in the cochleae of noise-exposed mice. Given the known binding of oseltamivir to viral neuraminidase, we tested whether the drug would inhibit the activity of mammalian neuraminidases. Cochlear explants were treated with N-acetyl-2,3-dehydro-2-deoxyneuraminic acid (DANA), a pan-selective mammalian neuraminidase inhibitor, or zanamivir, an older antiviral drug that has greater off-target affinity for mammalian neuraminidases than oseltamivir (Figure 4A–D).<span><sup>7</sup></span> Neither DANA nor zanamivir cotreatments reduced OHCs death relative to cisplatin alone (Figure 4A–D), indicating that oseltamivir's otoprotection is not mediated through neuraminidase inhibition.</p><p>Next, we submitted the chemical structures of the pro-drug, oseltamivir phosphate, and its active metabolite, oseltamivir carboxylate, to the drug target prediction server based on binding data, SuperPRED.<span><sup>8</sup></span> ERK2 and NF-kB p105 were top hits for both compounds at a probability coefficient exceeding .95 (Figure 4E,F). In cochlear mouse explants, mean pERK fluorescence was significantly reduced with cotreatment of 3 µM oseltamivir phosphate compared to cisplatin alone (Figure 4G,H).</p><p>To test whether oseltamivir decreases inflammation following noise exposure, mice were exposed to 100 dB SPL noise for 2 h and their cochleae were collected 4 days post-exposure (Figure 4I). Noise-exposed mice had a significantly higher average of CD45-positive cells per cochlear section (37) compared to non-noise exposed carrier (16) or oseltamivir (14) treated mice. Mice cotreated with 100 mg/kg oseltamivir for 3 days twice daily had a significant reduction in the number of CD45-positive cells per cochlear section (25) compared to noise alone mice (Figure 4J,K).</p><p>Oseltamivir is a widely used antiviral drug with a good safety profile.<span><sup>9</sup></span> Here, we measured significant protection from hearing loss with a dose of 10 mg/kg given twice a day, which is 66% of the mouse equivalent of the standard adult influenza dose.<span><sup>10</sup></span> These results demonstrate promising preclinical data that oseltamivir can be repurposed to protect against cisplatin and noise-induced hearing loss.</p><p>Tal Teitz, Duane Currier, Jian Zuo and Taosheng Chen designed and performed the cell-based screens. Matthew A. Ingersoll and Richard D. Lutze performed the in vivo cisplatin experiments. Emma J. Sailor-Longsworth and Regina G. Kelmann performed the in vivo noise exposure experiments. Matthew A. Ingersoll performed cochlear dissections, outer hair cell and Ctbp2 counts. Emma J. Sailor-Longsworth, Matthew A. Ingersoll and Kristina Ly performed cochlear explants experiments. Emma J. Sailor-Longsworth, Regina G. Kelmann, Matthew A. Ingersoll and Richard D. Lutze analysed ABR and DPOAE data. Richard D. Lutze and Regina G. Kelmann performed and imaged the cochlear CD45-stained cryosections. Richard D. Lutze performed the cisplatin interference testing in tumour cell lines. Emma J. Sailor-Longsworth, Matthew A. Ingersoll, Richard D. Lutze, Regina G. Kelmann, Kristina Ly and Tal Teitz were involved in the analysis of data and the design of the study. Emma J. Sailor-Longsworth, Richard D. Lutze, Kristina Ly, Regina G. Kelmann, Matthew A. Ingersoll and Tal Teitz wrote the manuscript with input from all authors.</p><p>T.T. and J.Z. are inventors of provisional patent applications filed for the use of oseltamivir in hearing protection #18/129267, #18/106918, and are co-founders of Ting Therapeutics LLC. All other authors declare that they have no competing interests.</p><p>The research was funded by the following grants: Department of Defense Award #W81XWH-21-1-0696 (grant RH200032), LB 506 Award from Nebraska State, Department of Health and Human Services, Cancer and Smoking Disease Research Program, National Institutes of Health NIDCD (grant 1R01DC018850) and American Hearing Research Foundation 2020 grant to Tal Teitz. This investigation was conducted in facilities constructed with support from Research Facilities Improvement Program (G20 RR024001-01) from the National Center for Research Resources, NIH. The research was partially conducted at the Auditory and Vestibular Technology Core at Creighton University, Omaha, NE (RRID: SCR_023866). This facility is supported by the Creighton University School of Medicine and grants GM103427 and GM139762 from the National Institute of General Medical Science (NIGMS), a component of the National Institutes of Health (NIH). IBIF was constructed with support from grants from the National Center for Research Resources (RR016469) and the NIGMS (GM103427). This is manuscript #1076 from The Scintillon Research Institute. This investigation is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources, NIGMS or NIH.</p>","PeriodicalId":10189,"journal":{"name":"Clinical and Translational Medicine","volume":"14 8","pages":""},"PeriodicalIF":6.8000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctm2.1803","citationCount":"0","resultStr":"{\"title\":\"Oseltamivir (Tamiflu), a commonly prescribed antiviral drug, mitigates hearing loss in mice\",\"authors\":\"Emma J. Sailor-Longsworth, Richard D. Lutze, Matthew A. Ingersoll, Regina G. Kelmann, Kristina Ly, Duane Currier, Taosheng Chen, Jian Zuo, Tal Teitz\",\"doi\":\"10.1002/ctm2.1803\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Dear Editor,</p><p>Hearing loss affects up to 10% of people worldwide and therapeutic interventions are desperately needed. Noise exposure and chemotherapy treatments are leading causes of this impairment, but currently there is only one FDA-approved drug for a subgroup of cisplatin-treated cancer patients.<span><sup>1, 2</sup></span> Hearing loss can arise from damage to many different inner ear cell types with outer hair cell (OHC) and synaptic dysfunction as two of the most common aetiologies of hearing loss.<span><sup>2-4</sup></span> Drug repurposing is a strategy for addressing unmet medical needs that can be quicker and more cost-effective than traditional drug development.<span><sup>3</sup></span> Here, we performed unbiased cell-based screens of 1300 FDA-approved drugs and tested our top candidate oseltamivir phosphate (brand name Tamiflu), a common influenza antiviral drug, in established cisplatin- and noise-induced hearing loss animal models. Our results support oseltamivir as a promising otoprotective therapeutic candidate for both cisplatin chemotherapy and traumatic noise exposure.</p><p>Oseltamivir phosphate and its active form, oseltamivir carboxylate, protect against cisplatin-induced hair cell loss in mouse cochlear explants without interfering with cisplatin's tumour killing efficacy in tumour cell lines. The prodrug, oseltamivir phosphate, tested at a dose of 3 µM, was a top hit in high-throughput screens reducing 95% of the caspase-3/7 cell death activity of cisplatin-treated cells.<span><sup>3, 4</sup></span> In mouse P3 cochlear explants, the prodrug, oseltamivir phosphate, protected from cisplatin-induced OHC death with an EC<sub>50</sub> of 450 nM (Figure 1A,D), while the active antiviral drug, oseltamivir carboxylate (Figure 1B), had a similar EC<sub>50</sub> of 505 nM (Figure 1C,E). Importantly, oseltamivir cotreatment in three small cell lung carcinoma and three neuroblastoma cell lines did not interfere with cisplatin's ability to kill tumour cells (Figure 1F–K).</p><p>Oseltamivir protects mice from cisplatin ototoxicity after a single, high dose of cisplatin and in a clinically relevant, multicycle cisplatin protocol. Adult FVB/NJ mice were treated orally with 50 mg/kg oseltamivir phosphate, 45 min before one dose of 30 mg/kg cisplatin (Figure 2A). We measured auditory brainstem response (ABR) as a test of hearing function. ABR measures nerve electrical activities from the cochleae to the brain. The ABR threshold is the lowest decibel sound pressure level (dB SPL) an animal can hear at. Mice cotreated with oseltamivir and cisplatin had 15 dB lower ABR threshold shifts at the 32 kHz region and displayed reduction in OHC death at the middle and basal cochlear regions compared to cisplatin-treated mice (Figure 2B–E). Utilising a clinically relevant multicycle cisplatin mouse model that mimics cisplatin treatment in humans (Figure 2F),<span><sup>4-6</sup></span> mice were treated orally with 50, 10 or 2 mg/kg oseltamivir, 45 min before the cisplatin treatment in the morning and 12 h later for three consecutive days. An amount of 3 mg/kg of cisplatin was administered via intraperitoneal injection. Mice cotreated with 50 and 10 mg/kg oseltamivir had significantly lower ABR threshold shifts at the 16 and 32 kHz regions, while 2 mg/kg oseltamivir treatment had no difference compared to cisplatin alone (Figure 2G,H). The 50 and 10 mg/kg oseltamivir cotreated mice with cisplatin had significantly higher ABR wave 1 amplitudes at 90 dB (Figure 2L), but no reduction in distortion product otoacoustic emission (DPOAE) threshold shifts (Figure 2I). The 50 and 10 mg/kg oseltamivir cotreatments conferred a significant reduction in OHCs loss (Figure 2J,K) and no significant difference in weight loss compared to cisplatin alone (Figure 2M).</p><p>Oral oseltamivir therapy protects against noise-induced ABR threshold shifts and cochlear synaptopathy. Mice, females or males, who received 100 mg/kg oseltamivir phosphate 24 h after noise exposure (Figure 3A) exhibited significantly reduced ABR threshold shifts relative to carrier-treated mice (Figure 3B–D). Mice that received 50 mg/kg oseltamivir had significant protection at 8 kHz (Figure 3E). No ABR protection was observed in the 10 mg/kg oseltamivir treatment group (Figure 3F). No treatment group exhibited protection from DPOAE threshold shifts (Figure 3G–I). Three-day oseltamivir treatment was sufficient for maximum otoprotective effects when initiated up to 24 h after 100 dB, 2-h noise exposure, but no protection was achieved with 106 dB, 2-h noise insult (Figure S1).</p><p>Mice treated with 100 mg/kg oseltamivir portrayed significantly higher average ABR wave 1 amplitude at 90 and 80 dB SPL and higher number of Ctbp2 inner hair cell synaptic puncta relative to carrier-treated noise exposed mice (Figure 3J–L).</p><p>Oseltamivir cisplatin otoprotection is partially mediated through inhibition of pERK protein levels and is associated with reduction in CD45-positive immune cells in the cochleae of noise-exposed mice. Given the known binding of oseltamivir to viral neuraminidase, we tested whether the drug would inhibit the activity of mammalian neuraminidases. Cochlear explants were treated with N-acetyl-2,3-dehydro-2-deoxyneuraminic acid (DANA), a pan-selective mammalian neuraminidase inhibitor, or zanamivir, an older antiviral drug that has greater off-target affinity for mammalian neuraminidases than oseltamivir (Figure 4A–D).<span><sup>7</sup></span> Neither DANA nor zanamivir cotreatments reduced OHCs death relative to cisplatin alone (Figure 4A–D), indicating that oseltamivir's otoprotection is not mediated through neuraminidase inhibition.</p><p>Next, we submitted the chemical structures of the pro-drug, oseltamivir phosphate, and its active metabolite, oseltamivir carboxylate, to the drug target prediction server based on binding data, SuperPRED.<span><sup>8</sup></span> ERK2 and NF-kB p105 were top hits for both compounds at a probability coefficient exceeding .95 (Figure 4E,F). In cochlear mouse explants, mean pERK fluorescence was significantly reduced with cotreatment of 3 µM oseltamivir phosphate compared to cisplatin alone (Figure 4G,H).</p><p>To test whether oseltamivir decreases inflammation following noise exposure, mice were exposed to 100 dB SPL noise for 2 h and their cochleae were collected 4 days post-exposure (Figure 4I). Noise-exposed mice had a significantly higher average of CD45-positive cells per cochlear section (37) compared to non-noise exposed carrier (16) or oseltamivir (14) treated mice. Mice cotreated with 100 mg/kg oseltamivir for 3 days twice daily had a significant reduction in the number of CD45-positive cells per cochlear section (25) compared to noise alone mice (Figure 4J,K).</p><p>Oseltamivir is a widely used antiviral drug with a good safety profile.<span><sup>9</sup></span> Here, we measured significant protection from hearing loss with a dose of 10 mg/kg given twice a day, which is 66% of the mouse equivalent of the standard adult influenza dose.<span><sup>10</sup></span> These results demonstrate promising preclinical data that oseltamivir can be repurposed to protect against cisplatin and noise-induced hearing loss.</p><p>Tal Teitz, Duane Currier, Jian Zuo and Taosheng Chen designed and performed the cell-based screens. Matthew A. Ingersoll and Richard D. Lutze performed the in vivo cisplatin experiments. Emma J. Sailor-Longsworth and Regina G. Kelmann performed the in vivo noise exposure experiments. Matthew A. Ingersoll performed cochlear dissections, outer hair cell and Ctbp2 counts. Emma J. Sailor-Longsworth, Matthew A. Ingersoll and Kristina Ly performed cochlear explants experiments. Emma J. Sailor-Longsworth, Regina G. Kelmann, Matthew A. Ingersoll and Richard D. Lutze analysed ABR and DPOAE data. Richard D. Lutze and Regina G. Kelmann performed and imaged the cochlear CD45-stained cryosections. Richard D. Lutze performed the cisplatin interference testing in tumour cell lines. Emma J. Sailor-Longsworth, Matthew A. Ingersoll, Richard D. Lutze, Regina G. Kelmann, Kristina Ly and Tal Teitz were involved in the analysis of data and the design of the study. Emma J. Sailor-Longsworth, Richard D. Lutze, Kristina Ly, Regina G. Kelmann, Matthew A. Ingersoll and Tal Teitz wrote the manuscript with input from all authors.</p><p>T.T. and J.Z. are inventors of provisional patent applications filed for the use of oseltamivir in hearing protection #18/129267, #18/106918, and are co-founders of Ting Therapeutics LLC. All other authors declare that they have no competing interests.</p><p>The research was funded by the following grants: Department of Defense Award #W81XWH-21-1-0696 (grant RH200032), LB 506 Award from Nebraska State, Department of Health and Human Services, Cancer and Smoking Disease Research Program, National Institutes of Health NIDCD (grant 1R01DC018850) and American Hearing Research Foundation 2020 grant to Tal Teitz. This investigation was conducted in facilities constructed with support from Research Facilities Improvement Program (G20 RR024001-01) from the National Center for Research Resources, NIH. The research was partially conducted at the Auditory and Vestibular Technology Core at Creighton University, Omaha, NE (RRID: SCR_023866). This facility is supported by the Creighton University School of Medicine and grants GM103427 and GM139762 from the National Institute of General Medical Science (NIGMS), a component of the National Institutes of Health (NIH). IBIF was constructed with support from grants from the National Center for Research Resources (RR016469) and the NIGMS (GM103427). This is manuscript #1076 from The Scintillon Research Institute. This investigation is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources, NIGMS or NIH.</p>\",\"PeriodicalId\":10189,\"journal\":{\"name\":\"Clinical and Translational Medicine\",\"volume\":\"14 8\",\"pages\":\"\"},\"PeriodicalIF\":6.8000,\"publicationDate\":\"2024-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctm2.1803\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.1803\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.1803","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Oseltamivir (Tamiflu), a commonly prescribed antiviral drug, mitigates hearing loss in mice
Dear Editor,
Hearing loss affects up to 10% of people worldwide and therapeutic interventions are desperately needed. Noise exposure and chemotherapy treatments are leading causes of this impairment, but currently there is only one FDA-approved drug for a subgroup of cisplatin-treated cancer patients.1, 2 Hearing loss can arise from damage to many different inner ear cell types with outer hair cell (OHC) and synaptic dysfunction as two of the most common aetiologies of hearing loss.2-4 Drug repurposing is a strategy for addressing unmet medical needs that can be quicker and more cost-effective than traditional drug development.3 Here, we performed unbiased cell-based screens of 1300 FDA-approved drugs and tested our top candidate oseltamivir phosphate (brand name Tamiflu), a common influenza antiviral drug, in established cisplatin- and noise-induced hearing loss animal models. Our results support oseltamivir as a promising otoprotective therapeutic candidate for both cisplatin chemotherapy and traumatic noise exposure.
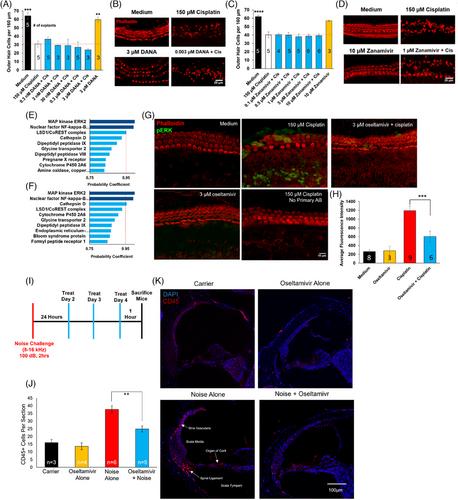
Oseltamivir phosphate and its active form, oseltamivir carboxylate, protect against cisplatin-induced hair cell loss in mouse cochlear explants without interfering with cisplatin's tumour killing efficacy in tumour cell lines. The prodrug, oseltamivir phosphate, tested at a dose of 3 µM, was a top hit in high-throughput screens reducing 95% of the caspase-3/7 cell death activity of cisplatin-treated cells.3, 4 In mouse P3 cochlear explants, the prodrug, oseltamivir phosphate, protected from cisplatin-induced OHC death with an EC50 of 450 nM (Figure 1A,D), while the active antiviral drug, oseltamivir carboxylate (Figure 1B), had a similar EC50 of 505 nM (Figure 1C,E). Importantly, oseltamivir cotreatment in three small cell lung carcinoma and three neuroblastoma cell lines did not interfere with cisplatin's ability to kill tumour cells (Figure 1F–K).
Oseltamivir protects mice from cisplatin ototoxicity after a single, high dose of cisplatin and in a clinically relevant, multicycle cisplatin protocol. Adult FVB/NJ mice were treated orally with 50 mg/kg oseltamivir phosphate, 45 min before one dose of 30 mg/kg cisplatin (Figure 2A). We measured auditory brainstem response (ABR) as a test of hearing function. ABR measures nerve electrical activities from the cochleae to the brain. The ABR threshold is the lowest decibel sound pressure level (dB SPL) an animal can hear at. Mice cotreated with oseltamivir and cisplatin had 15 dB lower ABR threshold shifts at the 32 kHz region and displayed reduction in OHC death at the middle and basal cochlear regions compared to cisplatin-treated mice (Figure 2B–E). Utilising a clinically relevant multicycle cisplatin mouse model that mimics cisplatin treatment in humans (Figure 2F),4-6 mice were treated orally with 50, 10 or 2 mg/kg oseltamivir, 45 min before the cisplatin treatment in the morning and 12 h later for three consecutive days. An amount of 3 mg/kg of cisplatin was administered via intraperitoneal injection. Mice cotreated with 50 and 10 mg/kg oseltamivir had significantly lower ABR threshold shifts at the 16 and 32 kHz regions, while 2 mg/kg oseltamivir treatment had no difference compared to cisplatin alone (Figure 2G,H). The 50 and 10 mg/kg oseltamivir cotreated mice with cisplatin had significantly higher ABR wave 1 amplitudes at 90 dB (Figure 2L), but no reduction in distortion product otoacoustic emission (DPOAE) threshold shifts (Figure 2I). The 50 and 10 mg/kg oseltamivir cotreatments conferred a significant reduction in OHCs loss (Figure 2J,K) and no significant difference in weight loss compared to cisplatin alone (Figure 2M).
Oral oseltamivir therapy protects against noise-induced ABR threshold shifts and cochlear synaptopathy. Mice, females or males, who received 100 mg/kg oseltamivir phosphate 24 h after noise exposure (Figure 3A) exhibited significantly reduced ABR threshold shifts relative to carrier-treated mice (Figure 3B–D). Mice that received 50 mg/kg oseltamivir had significant protection at 8 kHz (Figure 3E). No ABR protection was observed in the 10 mg/kg oseltamivir treatment group (Figure 3F). No treatment group exhibited protection from DPOAE threshold shifts (Figure 3G–I). Three-day oseltamivir treatment was sufficient for maximum otoprotective effects when initiated up to 24 h after 100 dB, 2-h noise exposure, but no protection was achieved with 106 dB, 2-h noise insult (Figure S1).
Mice treated with 100 mg/kg oseltamivir portrayed significantly higher average ABR wave 1 amplitude at 90 and 80 dB SPL and higher number of Ctbp2 inner hair cell synaptic puncta relative to carrier-treated noise exposed mice (Figure 3J–L).
Oseltamivir cisplatin otoprotection is partially mediated through inhibition of pERK protein levels and is associated with reduction in CD45-positive immune cells in the cochleae of noise-exposed mice. Given the known binding of oseltamivir to viral neuraminidase, we tested whether the drug would inhibit the activity of mammalian neuraminidases. Cochlear explants were treated with N-acetyl-2,3-dehydro-2-deoxyneuraminic acid (DANA), a pan-selective mammalian neuraminidase inhibitor, or zanamivir, an older antiviral drug that has greater off-target affinity for mammalian neuraminidases than oseltamivir (Figure 4A–D).7 Neither DANA nor zanamivir cotreatments reduced OHCs death relative to cisplatin alone (Figure 4A–D), indicating that oseltamivir's otoprotection is not mediated through neuraminidase inhibition.
Next, we submitted the chemical structures of the pro-drug, oseltamivir phosphate, and its active metabolite, oseltamivir carboxylate, to the drug target prediction server based on binding data, SuperPRED.8 ERK2 and NF-kB p105 were top hits for both compounds at a probability coefficient exceeding .95 (Figure 4E,F). In cochlear mouse explants, mean pERK fluorescence was significantly reduced with cotreatment of 3 µM oseltamivir phosphate compared to cisplatin alone (Figure 4G,H).
To test whether oseltamivir decreases inflammation following noise exposure, mice were exposed to 100 dB SPL noise for 2 h and their cochleae were collected 4 days post-exposure (Figure 4I). Noise-exposed mice had a significantly higher average of CD45-positive cells per cochlear section (37) compared to non-noise exposed carrier (16) or oseltamivir (14) treated mice. Mice cotreated with 100 mg/kg oseltamivir for 3 days twice daily had a significant reduction in the number of CD45-positive cells per cochlear section (25) compared to noise alone mice (Figure 4J,K).
Oseltamivir is a widely used antiviral drug with a good safety profile.9 Here, we measured significant protection from hearing loss with a dose of 10 mg/kg given twice a day, which is 66% of the mouse equivalent of the standard adult influenza dose.10 These results demonstrate promising preclinical data that oseltamivir can be repurposed to protect against cisplatin and noise-induced hearing loss.
Tal Teitz, Duane Currier, Jian Zuo and Taosheng Chen designed and performed the cell-based screens. Matthew A. Ingersoll and Richard D. Lutze performed the in vivo cisplatin experiments. Emma J. Sailor-Longsworth and Regina G. Kelmann performed the in vivo noise exposure experiments. Matthew A. Ingersoll performed cochlear dissections, outer hair cell and Ctbp2 counts. Emma J. Sailor-Longsworth, Matthew A. Ingersoll and Kristina Ly performed cochlear explants experiments. Emma J. Sailor-Longsworth, Regina G. Kelmann, Matthew A. Ingersoll and Richard D. Lutze analysed ABR and DPOAE data. Richard D. Lutze and Regina G. Kelmann performed and imaged the cochlear CD45-stained cryosections. Richard D. Lutze performed the cisplatin interference testing in tumour cell lines. Emma J. Sailor-Longsworth, Matthew A. Ingersoll, Richard D. Lutze, Regina G. Kelmann, Kristina Ly and Tal Teitz were involved in the analysis of data and the design of the study. Emma J. Sailor-Longsworth, Richard D. Lutze, Kristina Ly, Regina G. Kelmann, Matthew A. Ingersoll and Tal Teitz wrote the manuscript with input from all authors.
T.T. and J.Z. are inventors of provisional patent applications filed for the use of oseltamivir in hearing protection #18/129267, #18/106918, and are co-founders of Ting Therapeutics LLC. All other authors declare that they have no competing interests.
The research was funded by the following grants: Department of Defense Award #W81XWH-21-1-0696 (grant RH200032), LB 506 Award from Nebraska State, Department of Health and Human Services, Cancer and Smoking Disease Research Program, National Institutes of Health NIDCD (grant 1R01DC018850) and American Hearing Research Foundation 2020 grant to Tal Teitz. This investigation was conducted in facilities constructed with support from Research Facilities Improvement Program (G20 RR024001-01) from the National Center for Research Resources, NIH. The research was partially conducted at the Auditory and Vestibular Technology Core at Creighton University, Omaha, NE (RRID: SCR_023866). This facility is supported by the Creighton University School of Medicine and grants GM103427 and GM139762 from the National Institute of General Medical Science (NIGMS), a component of the National Institutes of Health (NIH). IBIF was constructed with support from grants from the National Center for Research Resources (RR016469) and the NIGMS (GM103427). This is manuscript #1076 from The Scintillon Research Institute. This investigation is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources, NIGMS or NIH.
期刊介绍:
Clinical and Translational Medicine (CTM) is an international, peer-reviewed, open-access journal dedicated to accelerating the translation of preclinical research into clinical applications and fostering communication between basic and clinical scientists. It highlights the clinical potential and application of various fields including biotechnologies, biomaterials, bioengineering, biomarkers, molecular medicine, omics science, bioinformatics, immunology, molecular imaging, drug discovery, regulation, and health policy. With a focus on the bench-to-bedside approach, CTM prioritizes studies and clinical observations that generate hypotheses relevant to patients and diseases, guiding investigations in cellular and molecular medicine. The journal encourages submissions from clinicians, researchers, policymakers, and industry professionals.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
