{"title":"一例伪装成自身免疫性肝炎的内脏利什曼病。","authors":"Vinny Ea, Brigitte Papa, Rimma Goldberg","doi":"10.5694/mja2.52412","DOIUrl":null,"url":null,"abstract":"<p>A 72-year-old man with a history of well controlled type 2 diabetes was admitted to a tertiary metropolitan hospital for investigation of fevers, night sweats and unintentional weight loss of 18 kg over six months. He had pancytopenia with no symptoms or signs to suggest a focal infection, malignancy or rheumatological disease. Prior outpatient investigation findings revealed mild splenomegaly, with a normal bone marrow aspirate and positron emission tomography scan. At its nadir, the haemoglobin level was 106 g/L (reference interval [RI], 125–175 g/L), white cell count 1.9 × 10<sup>9</sup>/L (RI, 4.0–11.0 × 10<sup>9</sup>/L), neutrophil count 1.2 × 10<sup>9</sup>/L (RI, 2.00–8.00 × 10<sup>9</sup>/L) and platelets 120 × 10<sup>9</sup>/L (RI, 150–450 × 10<sup>9</sup>/L). Notably, liver function test results were mildly elevated in a mixed pattern with alkaline phosphatase 138 U/L (RI, 30–110 U/L), γ-glutamyl transferase 605 U/L (RI, 5–50 U/L) and alanine aminotransferase 78 U/L (RI, 5–40 U/L), with associated antinuclear antibody titre of more than 1280 (RI, < 160), and an elevated immunoglobulin G level of 38.6 g/L (RI, 7.5–15.6 g/L). Pertinent negative results included negative human immunodeficiency virus (HIV) and viral hepatitis serology, and negative anti-smooth muscle and anti-liver–kidney microsomal antibodies. Given these findings and the ongoing diagnostic dilemma, a liver biopsy was performed, showing mild interface hepatitis and lymphoplasmacytic infiltrate in the portal tracts (Box 1), and leading to a probable diagnosis of autoimmune hepatitis. Administration of azathioprine 25 mg and prednisolone 40 mg daily was initiated and the patient was discharged following improvement of his liver function test results.</p><p>The patient re-presented two weeks later due to worsening night sweats with no new localising symptoms and was found to have febrile neutropenia (neutrophil count, 0.4 × 10<sup>9</sup>/L). Administration of empiric antibiotics was started, and azathioprine was stopped due to possible contribution to worsening myelosuppression. As the patient was born in coastal Greece and had travelled there two years prior, leishmaniasis was raised as a differential diagnosis. A repeat bone marrow aspirate revealed <i>Leishmania</i> amastigotes under microscopy (Box 2) and polymerase chain reaction (PCR) testing was positive for <i>Leishmania donovani</i> complex. The patient was treated with intravenous liposomal amphotericin 3 mg/kg/dose on Days 1–5, Day 14 and Day 21, which led to resolution of symptoms and pancytopenia six weeks after treatment.</p><p>Visceral leishmaniasis is a vector-borne zoonotic disease primarily caused by parasites of the <i>L. donovani</i> complex (includes <i>L. donovani</i> and <i>Leishmania infantum</i>) and is transmitted via infected sandflies.<span><sup>1</sup></span> Globally, visceral leishmaniasis features on the World Health Organization list of neglected tropical diseases, with a significant burden in tropical and subtropical regions, including Northern Africa, South America, Western Asia, southern Europe and the Mediterranean.<span><sup>1, 2</sup></span> In Australia, the only native <i>Leishmania</i> species is <i>Leishmania australiensis</i>, which occurs in macropods (eg, kangaroos, wallabies, wallaroos) and is not known to cause human disease. Consequently, all reported cases have occurred in travellers from endemic regions.<span><sup>3</sup></span></p><p>Visceral leishmaniasis usually presents with an insidious onset of constitutional symptoms, pancytopenia, hepatomegaly and splenomegaly (which may be massive), due to replication of parasites in the reticuloendothelial system.<span><sup>4</sup></span> Complications range from bleeding, hepatic dysfunction and neutropenic infections to disseminated intravascular coagulation and haemophagocytic lymphohistiocytosis. Untreated disease is associated with a high mortality rate.<span><sup>5</sup></span> The incubation period is usually months, although may range from a few weeks to several years. In this case, the patient had not travelled to Greece or other endemic areas in two years, reflecting a prolonged incubation period. This highlights the importance of obtaining an extended travel history for diagnoses, as well as in screening for latent infections before commencing immunosuppressive medications.</p><p>Traditionally, definitive diagnosis of visceral leishmaniasis requires visualisation of parasites on a tissue smear of bone marrow or splenic aspirates. However, sensitivity depends on thorough microbiological examination,<span><sup>6</sup></span> and biopsies may be associated with procedural risks such as splenic haemorrhage, particularly given the increased bleeding tendency in visceral leishmaniasis. Alternatively, molecular testing with PCR of peripheral blood, bone marrow and splenic tissue is sensitive, exceeding microbiological examination in some studies,<span><sup>7</sup></span> although this approach is limited to specialised laboratories. Serological diagnosis using the rK39 antigen also carries reasonable sensitivity. In endemic regions, PCR and serological testing may be less specific as subclinical carriers and treated cases may express positive results.<span><sup>8</sup></span> Additionally, serology has limited value in immunocompromised patients who do not mount a serological response to leishmaniasis, although this is not a concern for PCR testing. Overall, in non-endemic regions, PCR testing with supportive clinical and epidemiological features is an appropriate modality for diagnosis.</p><p>In this patient, the diagnosis of visceral leishmaniasis was confounded by an initial diagnosis of autoimmune hepatitis. The association between visceral leishmaniasis with autoantibodies, hypergammaglobulinemia and histopathological features mimicking autoimmune hepatitis has been previously described in the literature.<span><sup>9, 10</sup></span> Proposed mechanisms include tissue destruction by parasites leading to release of tissue antigens and inducing autoreactivity with autoantibody production; and stimulation of polyclonal B cell activation in visceral leishmaniasis leading to hypergammaglobulinemia.<span><sup>11</sup></span> Due to these immunological phenomena, visceral leishmaniasis has also been shown to mimic other autoimmune diseases, including systemic lupus erythematosus.<span><sup>10</sup></span> Mistreatment with immunosuppressive therapy may be detrimental, potentially leading to worsening of visceral leishmaniasis symptoms and precipitating secondary bacterial infections.</p><p>Treatment of visceral leishmaniasis varies regionally due to drug susceptibility, availability and cost, with liposomal amphotericin B being the preferred agent in resource-rich countries based on its superior antimicrobial efficacy and safety profile. Further treatment considerations are also required for immunocompromised individuals, especially in HIV–<i>L. donovani</i> complex co-infection whereby cellular immunity is depleted, and antimicrobial therapy may be inadequate without immune reconstitution. There are no guidelines for the management of visceral leishmaniasis in Australia and our treatment regimen reflects that of North American guidelines.<span><sup>12</sup></span></p><p>In summary, visceral leishmaniasis is seldom found in Australia and remains a rare differential diagnosis for pancytopenia and pyrexia of unknown origin. However, with increasing globalisation, this diagnosis should be entertained in people arriving or returning from endemic countries.</p><p>Open access publishing facilitated by Monash University, as part of the Wiley - Monash University agreement via the Council of Australian University Librarians.</p><p>The patient gave written consent for publication.</p><p>No relevant disclosures.</p><p>Not commissioned; externally peer reviewed.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 6","pages":"299-301"},"PeriodicalIF":8.5000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52412","citationCount":"0","resultStr":"{\"title\":\"A case of visceral leishmaniasis masquerading as autoimmune hepatitis\",\"authors\":\"Vinny Ea, Brigitte Papa, Rimma Goldberg\",\"doi\":\"10.5694/mja2.52412\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 72-year-old man with a history of well controlled type 2 diabetes was admitted to a tertiary metropolitan hospital for investigation of fevers, night sweats and unintentional weight loss of 18 kg over six months. He had pancytopenia with no symptoms or signs to suggest a focal infection, malignancy or rheumatological disease. Prior outpatient investigation findings revealed mild splenomegaly, with a normal bone marrow aspirate and positron emission tomography scan. At its nadir, the haemoglobin level was 106 g/L (reference interval [RI], 125–175 g/L), white cell count 1.9 × 10<sup>9</sup>/L (RI, 4.0–11.0 × 10<sup>9</sup>/L), neutrophil count 1.2 × 10<sup>9</sup>/L (RI, 2.00–8.00 × 10<sup>9</sup>/L) and platelets 120 × 10<sup>9</sup>/L (RI, 150–450 × 10<sup>9</sup>/L). Notably, liver function test results were mildly elevated in a mixed pattern with alkaline phosphatase 138 U/L (RI, 30–110 U/L), γ-glutamyl transferase 605 U/L (RI, 5–50 U/L) and alanine aminotransferase 78 U/L (RI, 5–40 U/L), with associated antinuclear antibody titre of more than 1280 (RI, < 160), and an elevated immunoglobulin G level of 38.6 g/L (RI, 7.5–15.6 g/L). Pertinent negative results included negative human immunodeficiency virus (HIV) and viral hepatitis serology, and negative anti-smooth muscle and anti-liver–kidney microsomal antibodies. Given these findings and the ongoing diagnostic dilemma, a liver biopsy was performed, showing mild interface hepatitis and lymphoplasmacytic infiltrate in the portal tracts (Box 1), and leading to a probable diagnosis of autoimmune hepatitis. Administration of azathioprine 25 mg and prednisolone 40 mg daily was initiated and the patient was discharged following improvement of his liver function test results.</p><p>The patient re-presented two weeks later due to worsening night sweats with no new localising symptoms and was found to have febrile neutropenia (neutrophil count, 0.4 × 10<sup>9</sup>/L). Administration of empiric antibiotics was started, and azathioprine was stopped due to possible contribution to worsening myelosuppression. As the patient was born in coastal Greece and had travelled there two years prior, leishmaniasis was raised as a differential diagnosis. A repeat bone marrow aspirate revealed <i>Leishmania</i> amastigotes under microscopy (Box 2) and polymerase chain reaction (PCR) testing was positive for <i>Leishmania donovani</i> complex. The patient was treated with intravenous liposomal amphotericin 3 mg/kg/dose on Days 1–5, Day 14 and Day 21, which led to resolution of symptoms and pancytopenia six weeks after treatment.</p><p>Visceral leishmaniasis is a vector-borne zoonotic disease primarily caused by parasites of the <i>L. donovani</i> complex (includes <i>L. donovani</i> and <i>Leishmania infantum</i>) and is transmitted via infected sandflies.<span><sup>1</sup></span> Globally, visceral leishmaniasis features on the World Health Organization list of neglected tropical diseases, with a significant burden in tropical and subtropical regions, including Northern Africa, South America, Western Asia, southern Europe and the Mediterranean.<span><sup>1, 2</sup></span> In Australia, the only native <i>Leishmania</i> species is <i>Leishmania australiensis</i>, which occurs in macropods (eg, kangaroos, wallabies, wallaroos) and is not known to cause human disease. Consequently, all reported cases have occurred in travellers from endemic regions.<span><sup>3</sup></span></p><p>Visceral leishmaniasis usually presents with an insidious onset of constitutional symptoms, pancytopenia, hepatomegaly and splenomegaly (which may be massive), due to replication of parasites in the reticuloendothelial system.<span><sup>4</sup></span> Complications range from bleeding, hepatic dysfunction and neutropenic infections to disseminated intravascular coagulation and haemophagocytic lymphohistiocytosis. Untreated disease is associated with a high mortality rate.<span><sup>5</sup></span> The incubation period is usually months, although may range from a few weeks to several years. In this case, the patient had not travelled to Greece or other endemic areas in two years, reflecting a prolonged incubation period. This highlights the importance of obtaining an extended travel history for diagnoses, as well as in screening for latent infections before commencing immunosuppressive medications.</p><p>Traditionally, definitive diagnosis of visceral leishmaniasis requires visualisation of parasites on a tissue smear of bone marrow or splenic aspirates. However, sensitivity depends on thorough microbiological examination,<span><sup>6</sup></span> and biopsies may be associated with procedural risks such as splenic haemorrhage, particularly given the increased bleeding tendency in visceral leishmaniasis. Alternatively, molecular testing with PCR of peripheral blood, bone marrow and splenic tissue is sensitive, exceeding microbiological examination in some studies,<span><sup>7</sup></span> although this approach is limited to specialised laboratories. Serological diagnosis using the rK39 antigen also carries reasonable sensitivity. In endemic regions, PCR and serological testing may be less specific as subclinical carriers and treated cases may express positive results.<span><sup>8</sup></span> Additionally, serology has limited value in immunocompromised patients who do not mount a serological response to leishmaniasis, although this is not a concern for PCR testing. Overall, in non-endemic regions, PCR testing with supportive clinical and epidemiological features is an appropriate modality for diagnosis.</p><p>In this patient, the diagnosis of visceral leishmaniasis was confounded by an initial diagnosis of autoimmune hepatitis. The association between visceral leishmaniasis with autoantibodies, hypergammaglobulinemia and histopathological features mimicking autoimmune hepatitis has been previously described in the literature.<span><sup>9, 10</sup></span> Proposed mechanisms include tissue destruction by parasites leading to release of tissue antigens and inducing autoreactivity with autoantibody production; and stimulation of polyclonal B cell activation in visceral leishmaniasis leading to hypergammaglobulinemia.<span><sup>11</sup></span> Due to these immunological phenomena, visceral leishmaniasis has also been shown to mimic other autoimmune diseases, including systemic lupus erythematosus.<span><sup>10</sup></span> Mistreatment with immunosuppressive therapy may be detrimental, potentially leading to worsening of visceral leishmaniasis symptoms and precipitating secondary bacterial infections.</p><p>Treatment of visceral leishmaniasis varies regionally due to drug susceptibility, availability and cost, with liposomal amphotericin B being the preferred agent in resource-rich countries based on its superior antimicrobial efficacy and safety profile. Further treatment considerations are also required for immunocompromised individuals, especially in HIV–<i>L. donovani</i> complex co-infection whereby cellular immunity is depleted, and antimicrobial therapy may be inadequate without immune reconstitution. There are no guidelines for the management of visceral leishmaniasis in Australia and our treatment regimen reflects that of North American guidelines.<span><sup>12</sup></span></p><p>In summary, visceral leishmaniasis is seldom found in Australia and remains a rare differential diagnosis for pancytopenia and pyrexia of unknown origin. However, with increasing globalisation, this diagnosis should be entertained in people arriving or returning from endemic countries.</p><p>Open access publishing facilitated by Monash University, as part of the Wiley - Monash University agreement via the Council of Australian University Librarians.</p><p>The patient gave written consent for publication.</p><p>No relevant disclosures.</p><p>Not commissioned; externally peer reviewed.</p>\",\"PeriodicalId\":18214,\"journal\":{\"name\":\"Medical Journal of Australia\",\"volume\":\"221 6\",\"pages\":\"299-301\"},\"PeriodicalIF\":8.5000,\"publicationDate\":\"2024-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52412\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Journal of Australia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52412\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52412","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
A case of visceral leishmaniasis masquerading as autoimmune hepatitis
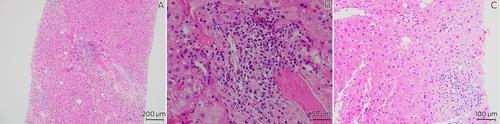
A 72-year-old man with a history of well controlled type 2 diabetes was admitted to a tertiary metropolitan hospital for investigation of fevers, night sweats and unintentional weight loss of 18 kg over six months. He had pancytopenia with no symptoms or signs to suggest a focal infection, malignancy or rheumatological disease. Prior outpatient investigation findings revealed mild splenomegaly, with a normal bone marrow aspirate and positron emission tomography scan. At its nadir, the haemoglobin level was 106 g/L (reference interval [RI], 125–175 g/L), white cell count 1.9 × 109/L (RI, 4.0–11.0 × 109/L), neutrophil count 1.2 × 109/L (RI, 2.00–8.00 × 109/L) and platelets 120 × 109/L (RI, 150–450 × 109/L). Notably, liver function test results were mildly elevated in a mixed pattern with alkaline phosphatase 138 U/L (RI, 30–110 U/L), γ-glutamyl transferase 605 U/L (RI, 5–50 U/L) and alanine aminotransferase 78 U/L (RI, 5–40 U/L), with associated antinuclear antibody titre of more than 1280 (RI, < 160), and an elevated immunoglobulin G level of 38.6 g/L (RI, 7.5–15.6 g/L). Pertinent negative results included negative human immunodeficiency virus (HIV) and viral hepatitis serology, and negative anti-smooth muscle and anti-liver–kidney microsomal antibodies. Given these findings and the ongoing diagnostic dilemma, a liver biopsy was performed, showing mild interface hepatitis and lymphoplasmacytic infiltrate in the portal tracts (Box 1), and leading to a probable diagnosis of autoimmune hepatitis. Administration of azathioprine 25 mg and prednisolone 40 mg daily was initiated and the patient was discharged following improvement of his liver function test results.
The patient re-presented two weeks later due to worsening night sweats with no new localising symptoms and was found to have febrile neutropenia (neutrophil count, 0.4 × 109/L). Administration of empiric antibiotics was started, and azathioprine was stopped due to possible contribution to worsening myelosuppression. As the patient was born in coastal Greece and had travelled there two years prior, leishmaniasis was raised as a differential diagnosis. A repeat bone marrow aspirate revealed Leishmania amastigotes under microscopy (Box 2) and polymerase chain reaction (PCR) testing was positive for Leishmania donovani complex. The patient was treated with intravenous liposomal amphotericin 3 mg/kg/dose on Days 1–5, Day 14 and Day 21, which led to resolution of symptoms and pancytopenia six weeks after treatment.
Visceral leishmaniasis is a vector-borne zoonotic disease primarily caused by parasites of the L. donovani complex (includes L. donovani and Leishmania infantum) and is transmitted via infected sandflies.1 Globally, visceral leishmaniasis features on the World Health Organization list of neglected tropical diseases, with a significant burden in tropical and subtropical regions, including Northern Africa, South America, Western Asia, southern Europe and the Mediterranean.1, 2 In Australia, the only native Leishmania species is Leishmania australiensis, which occurs in macropods (eg, kangaroos, wallabies, wallaroos) and is not known to cause human disease. Consequently, all reported cases have occurred in travellers from endemic regions.3
Visceral leishmaniasis usually presents with an insidious onset of constitutional symptoms, pancytopenia, hepatomegaly and splenomegaly (which may be massive), due to replication of parasites in the reticuloendothelial system.4 Complications range from bleeding, hepatic dysfunction and neutropenic infections to disseminated intravascular coagulation and haemophagocytic lymphohistiocytosis. Untreated disease is associated with a high mortality rate.5 The incubation period is usually months, although may range from a few weeks to several years. In this case, the patient had not travelled to Greece or other endemic areas in two years, reflecting a prolonged incubation period. This highlights the importance of obtaining an extended travel history for diagnoses, as well as in screening for latent infections before commencing immunosuppressive medications.
Traditionally, definitive diagnosis of visceral leishmaniasis requires visualisation of parasites on a tissue smear of bone marrow or splenic aspirates. However, sensitivity depends on thorough microbiological examination,6 and biopsies may be associated with procedural risks such as splenic haemorrhage, particularly given the increased bleeding tendency in visceral leishmaniasis. Alternatively, molecular testing with PCR of peripheral blood, bone marrow and splenic tissue is sensitive, exceeding microbiological examination in some studies,7 although this approach is limited to specialised laboratories. Serological diagnosis using the rK39 antigen also carries reasonable sensitivity. In endemic regions, PCR and serological testing may be less specific as subclinical carriers and treated cases may express positive results.8 Additionally, serology has limited value in immunocompromised patients who do not mount a serological response to leishmaniasis, although this is not a concern for PCR testing. Overall, in non-endemic regions, PCR testing with supportive clinical and epidemiological features is an appropriate modality for diagnosis.
In this patient, the diagnosis of visceral leishmaniasis was confounded by an initial diagnosis of autoimmune hepatitis. The association between visceral leishmaniasis with autoantibodies, hypergammaglobulinemia and histopathological features mimicking autoimmune hepatitis has been previously described in the literature.9, 10 Proposed mechanisms include tissue destruction by parasites leading to release of tissue antigens and inducing autoreactivity with autoantibody production; and stimulation of polyclonal B cell activation in visceral leishmaniasis leading to hypergammaglobulinemia.11 Due to these immunological phenomena, visceral leishmaniasis has also been shown to mimic other autoimmune diseases, including systemic lupus erythematosus.10 Mistreatment with immunosuppressive therapy may be detrimental, potentially leading to worsening of visceral leishmaniasis symptoms and precipitating secondary bacterial infections.
Treatment of visceral leishmaniasis varies regionally due to drug susceptibility, availability and cost, with liposomal amphotericin B being the preferred agent in resource-rich countries based on its superior antimicrobial efficacy and safety profile. Further treatment considerations are also required for immunocompromised individuals, especially in HIV–L. donovani complex co-infection whereby cellular immunity is depleted, and antimicrobial therapy may be inadequate without immune reconstitution. There are no guidelines for the management of visceral leishmaniasis in Australia and our treatment regimen reflects that of North American guidelines.12
In summary, visceral leishmaniasis is seldom found in Australia and remains a rare differential diagnosis for pancytopenia and pyrexia of unknown origin. However, with increasing globalisation, this diagnosis should be entertained in people arriving or returning from endemic countries.
Open access publishing facilitated by Monash University, as part of the Wiley - Monash University agreement via the Council of Australian University Librarians.
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
